NOTE: This was originally supposed to be a guest post for Kris Gunnars’ Authority Nutrition website, but in true Denise Minger fashion, the word count got out of control and we decided to dock it here instead. Voila! Just pretend you’re reading this on a blog far, far away, and that, for once in my life, I managed to be brief.
Ever since the “fat is bad” movement of the ‘90s morphed into our current era of carb-phobia, I’ve suspected the world would eventually turn its dietary lynch mob on protein—the only macronutrient not yet slandered by media headlines and hyperbolic Facebook memes.
Behold! The day has come.
Proteinaholic is the latest work of Dr. Garth Davis—a Houston-based weight loss surgeon whose personal and professional journey led him away from animal foods and down the fibrous, veggie-lined path of plant-based eating.
The book’s title isn’t quite as literal as a bevy of fumbling addicts slurping whey-protein shakes from paper bags, but in some ways, the image isn’t far off. Animal protein, according to Davis, is not the key to weight loss—but rather, a chief cause of our expanding waistlines. Far from making us healthier, it drives the progression of cancer, heart disease, diabetes, and other ailments crippling the Western world. Those who swap it out for the bounty of the plant kingdom are rewarded with greater longevity and disease protection, Davis argues.
Regardless of its scientific validity (which we’ll get to in a minute!), Proteinaholic is bound to make some waves. It’s stoking the flames of our next macronutrient-centric shift, bringing a new dietary villain to the fore, and adding ammo to the plant-based diet movement’s arsenal of “things that sound like proof.” Like The China Study, Proteinaholic is destined to become a go-to resource for those wanting scientific validation for veganism.
But that leads us to the question: does this book make a legitimate case against animal protein? Or is it an example of some kernels of truth swathed in selective interpretation and bias? Let the analytical games begin!
The Good
Although this critique will focus more on exposing inaccuracies than handing out gold-star stickers and back pats, Proteinaholic deserves some legitimate praise. The book hits the bullseye on more than a few occasions, offering valuable insights for readers of any dietary persuasion. As a small sample:
- The media as a major “contamination zone” in the river that carries science from the lab and to our ears. Davis helps clarify why new findings on health and disease seem to flip-flop on a daily basis: reporters are chiefly concerned with what’s new and exciting rather than what’s valid and reliable—leading to “anomalous findings … reported as medical breakthroughs, instead of outlier data that needs to be replicated with rigor” (pages 124-125).
- The inaccuracy of our most hyped-up model of diabetes: the tired pancreas theory, in which carbohydrates “spike our blood sugar and cause the pancreas to ultimately exhaust itself” (page 149). Davis justly critiques this model and explores the oft-overlooked role of fat accumulation and lipotoxicity in beta cell dysfunction. (Other bloggers, such as Ned Kock, have also reviewed the problems with the tired pancreas theory in more depth than we’ll have a chance to here.)
- The legitimate risks of a low-vegetable, meat-centric diet (especially meat of the red or processed variety) that health-conscious omnivores should probably take to heart. Many of these risks are context dependent and come with some important caveats, but in a nutshell: heme iron, gut microbiome shifts, excess methionine, and Neu5Gc all deserve serious consideration, as does the role of certain phytonutrients in neutralizing the byproducts of meat metabolism (pages 191-201). We’ll be taking a more nuanced look at these things later on!
 The likely health benefits of legumes. Although Davis mostly relies on observational studies here, it’s not for wont of controlled trials: an astounding amount of research exists on how legumes impact glycemic control, weight, the gut microbiome, and other health-pertinent issues. Davis dishes out valid criticisms of the legume-o-phobia pervading many low-carbohydrate and Paleo philosophies—noting that any links with weight gain are speculative, and their consumption seems associated with longevity on a global scale.
The likely health benefits of legumes. Although Davis mostly relies on observational studies here, it’s not for wont of controlled trials: an astounding amount of research exists on how legumes impact glycemic control, weight, the gut microbiome, and other health-pertinent issues. Davis dishes out valid criticisms of the legume-o-phobia pervading many low-carbohydrate and Paleo philosophies—noting that any links with weight gain are speculative, and their consumption seems associated with longevity on a global scale.- Our wonky, Twilight-Zoneish definition of “low fat.” Having recently blogged on this topic myself, Davis’s comments here are refreshingly familiar. In explaining the underwhelming results of most low-fat diet studies, he writes: “Typically what you will find is that the so-called low-fat diet group was never on a low-fat diet. Many of the studies showing that low-fat diets don’t lead to weight loss define low fat as 30 percent of calories, which is actually quite high” (page 180). Indeed, something special seems to happen when fat intake is capped around 10% of calories or less—a “magic zone” missed by nearly every study purporting to use a low-fat menu.
- The unwarranted demonization of carbs. Davis makes a compelling case that carbohydrates don’t play a central role in developing diabetes (page 152); that many junk foods we label “carbs” are actually equal parts carbohydrate and fat (like muffins and French fries) (page 71); and that it’s wildly inefficient for the body to store carbohydrates as fat, even in states of calorie excess (page 179).
- The government-industry connection simmering behind the scenes of national food guidelines. (What can I say? My own book was called Death by Food Pyramid—I was bound to swoon over this section, and swoon I did.) Davis nails the modern predicament in America: “The USDA is charged to not only make sure food is safe and good for you, but to also make sure that the businesses that produce food are profitable. … Worse yet, when conflict does arise between what is good for us and what is profitable, guess who wins?” (page 124). Likewise, he observes that the food industry itself thrives off of keeping the public confused, and that when it comes to funding and designing studies, it can afford a “much bigger megaphone than the honest nutritional scientists toiling away in their offices and labs” (page 121).

- The illogic behind loading up on saturated fat in the name of better health. This trend is reflected in the popularity of Bulletproof Coffee, “fat bomb” recipes, and other attempts to squeeze as much saturated fat as possible into every mouthward spoonful. Davis writes, “There’s an impossibly big leap between the statement that saturated fat may not be the prime reason for heart disease and the completely faulty conclusion that saturated fat is actually good for you” (page 88). I’d add that there’s a similar leap between saying saturated-fat-containing foods can have valuable nutrients and saying saturated fat itself is the thing that makes us healthier. With the exception of very specific types of saturated fat (like medium-chain triglycerides), there’s little evidence for the latter.
- The protective role of phytonutrients. In a rebellious-teen-like rampage to defy all tenets of conventional wisdom, some subsets of the low-carb movement (and other alternative diet groups) have become downright veggiephobic, believing plants really offer little benefit to our bodies. Davis rightfully explores the many benefits and disease-mediating roles of plant compounds—though it should be noted that eating meat and eating plants, even lots of plants, are far from mutually exclusive (pages 200-201).
Notice a pattern here? Ironically, the book’s most legitimate points don’t actually have anything to do with protein. Proteinaholic shines brightest when discussing low-fat diets, the benefits of plant phytochemicals, government and industry influences, occasional low-carb and Paleo fallacies, and non-protein components of animal foods. But, as we’ll soon see, it falters when it comes to supporting its actual thesis.
 Because this book has such an unusual combination of brilliant tangential points and weak central arguments, I’m whipping out the Level 5 Fine-Tooth Comb for what follows. By toppling the claims that can’t withstand scrutiny, we can be confident that what’s left standing is worth listening to—or at the very least, worth considering.
Because this book has such an unusual combination of brilliant tangential points and weak central arguments, I’m whipping out the Level 5 Fine-Tooth Comb for what follows. By toppling the claims that can’t withstand scrutiny, we can be confident that what’s left standing is worth listening to—or at the very least, worth considering.
I hope interested readers will grab a copy of Proteinaholic and dive into the references Davis generously links to on his website, approaching the work with a combination of open-mindedness, skepticism, and willingness to accept that bacon might not be a superfood. Which brings us to…
Factual Inaccuracies
Apart from the question of protein’s direct harmfulness (or lack thereof), Proteinaholic is scattered with easy-to-falsify inaccuracies. As just six examples:
1. RDA Confusion
CLAIM: In discussing America’s protein-noshing habits, Davis says the recommended daily allowances (RDAs) for protein—56 grams for men and 46 grams for women—are “actually optimal values, not minimal needs” (page 9). Anything higher than that should thus be considered excessive (and perhaps dangerous).
REALITY: The reverse is true! The RDA in general is defined as “the minimal amount to meet nutrient requirement, rather than an optimal level of nutrient intake” (1). For protein, the RDA gauges the “minimum protein intake necessary to avoid a progressive loss of lean body mass” (2). Likewise, the National Academies of Sciences states there was no upper level of protein intake “at which potential adverse effects … was identified” (3).
2. Lester Morrison: Low-Protein Pioneer, or Misrepresented Researcher?
CLAIM: Recounting the legacy of heart-disease researcher Dr. Lester Morrison, Davis writes (emphasis mine): “In the early 1950s, Morrison experimented by putting 50 of his sickest cardiac patients on a diet … low in animal products, high in fiber … while allowing 50 others to maintain their high-protein American diets. The results … were striking: by 1960, all the high-protein patients were dead, while 38 percent of the low-protein patients were still alive” (page 92).
 REALITY: Davis has it backwards here! Morrison’s exclusive concern was with fat intake—not protein or animal products. Because he made his patients nix all things lipid, the people on his test diet actually ended up eating more protein than the control group in order to fill the caloric void. Morrison himself described his experimental diet as “high-protein, low-fat,” with an average protein intake of 120 grams per day (4).
REALITY: Davis has it backwards here! Morrison’s exclusive concern was with fat intake—not protein or animal products. Because he made his patients nix all things lipid, the people on his test diet actually ended up eating more protein than the control group in order to fill the caloric void. Morrison himself described his experimental diet as “high-protein, low-fat,” with an average protein intake of 120 grams per day (4).
His permitted food list included (5):
- Lean meat, fish, and poultry
- Unlimited egg whites
- At least one pint of skim milk or buttermilk each day
- Skim-milk cheeses
- Soups made with skim milk
- Puddings made with skim milk
- Fruit whips made with egg whites
- Egg kisses
And on top of that, he prescribed an at-least-once-per-day drink containing skim milk, wheat germ, brewer’s yeast, and fruit “to provide additional protein in the diet” (4). In the end, the patients consuming this high-lean-animal-protein diet were the ones who thwarted an early death.
3. Do Nonhuman Primates Prove We Can Thrive on Low-Protein Diets?
CLAIM: Regarding Sylvester Graham, an early pioneer of the vegetarian movement (and originator of the much-loved Graham cracker), Davis says, “My favorite argument of Graham’s which has lost no validity over the years, is that orangutans and gorillas clearly prove that you don’t have to eat meat or dairy products to remain strong” (page 60).
REALITY: If this claim hasn’t lost any validity, it’s only because it had none to begin with. Unlike humans, orangutans and gorillas are fabulous hindgut fermenters—boasting huge colons full of cellulose-degrading bacteria that turn otherwise indigestible food into energy. (Think: twigs, bark, pith, and tough-as-leather foliage that make kale seem like tissue paper by comparison!)
Gorillas can wolf down over 40 pounds of vegetation in a day, and due to the sheer volume of food they consume, actually ingest an incredible amount of protein. Depending on the season, their protein intakes range from “similar to those recommended for humans” to “close to the maximum recommended for humans and similar to high-protein human weight-loss diets” (6). Humans, with our comparatively puny colons (and lack of all-day veggie buffets), don’t have the same ability to support gorilla-esque strength on a diet of leaves.
CLAIM: Continuing with the primate theme, Davis writes: “If you look at comparative anatomy of humans and other animals, we are much more related to chimps … What do chimps eat? Plants, plants, and more plants, with an occasional insect chaser. Very rarely do they eat other monkeys, and only in times of food scarcity” (page 100).
REALITY: This is a two-part blunder. One, although humans are definitely more anatomically similar to chimps than to, say, a duck or a set of Yahtzee dice, the differences we do possess are important ones. The chimpanzee gut is dominated by the colon, while the human gut is dominated by the small intestine—a proportional shift that indicates we’re better equipped to handle dense foods like meat and cooked starches than bulky plant roughage (7). So, comparing human anatomy to chimps’ actually undermines the idea that our optimal diet resembles theirs.

From Katharine Milton, 1999: “Nutritional characteristics of wild primate foods: do the diets of our closest living relatives have lessons for us?”
Two, chimpanzees are far from the peaceable, near-vegan herbivores Davis portrays them as! Chimps have a surprisingly intricate hunting ecology—patrolling the forest in slaughter-ready groups, scouting out meat even when other food is abundant, and in some populations (such as the chimps in Fongoli, Senegal) whittling tools out of branches to spear mongooses, bushbucks, baboons, vervet monkeys, patas monkeys, and bush babies (8, 9). In fact, chimps eat enough meat to leave isotopic animal-protein evidence in their hair keratin and bone collagen (10).
And as far as “occasional insect chasers” go? Creepy-crawlies are far from a minor dietary component! Chimpanzees derive significant levels of protein, iron, sodium, vitamin B12, copper, manganese, essential fatty acids, and other nutrients from invertebrates, and spend a disproportionate amount of time fishing for nutrient-dense ants and termites relative to higher-calorie foods (11, 12, 13).
4. Sugar, Inflammation, and Funding Foibles
CLAIM: To support the idea that sugar isn’t at the root of inflammation and disease (and to shift the blame back towards protein), Davis describes a study where participants consumed either sugar-sweetened or artificially sweetened drinks daily for 10 weeks. He relays the findings thusly (emphasis mine): “As would be expected, the sugary drink group consumed more calories and therefore gained more weight. But here’s what’s fascinating: even though they gained weight, they did not show any signs of increasing inflammation. The sugar seems to have no inflammatory effect at all …” (page 153).
 REALITY: The only way to draw this conclusion from the study is by not reading past the abstract. The full text paints a less pleasant picture (emphasis mine): “In conclusion, this study shows that, apart from causing weight gain and increasing blood pressure, a high consumption of sugar-sweetened drinks and foods may increase inflammatory activity in overweight subjects. This finding was independent of weight changes” (14).
REALITY: The only way to draw this conclusion from the study is by not reading past the abstract. The full text paints a less pleasant picture (emphasis mine): “In conclusion, this study shows that, apart from causing weight gain and increasing blood pressure, a high consumption of sugar-sweetened drinks and foods may increase inflammatory activity in overweight subjects. This finding was independent of weight changes” (14).
It’s also interesting Davis would cite this paper at all, given his earlier exposé on the influence of industry funding on research outcomes: the study was financially supported by Danisco Sugar!
5. Dietary Goals Consensus (Or Lack Thereof)
CLAIM: In explaining how the controversial 1977 Dietary Goals for the United States was altered to emphasize eating more lean meat instead of eating less total meat, Davis writes: “It’s not like there wasn’t support for the original recommendation [to reduce meat intake]. The American Society of Clinical Nutrition convened an unbiased committee to review the McGovern recommendations and found them completely valid” (page 69).
REALITY: This is a pretty rosy revision of history! In the American Society of Clinical Nutrition’s report, the only diet-disease theories the experts agreed on were that carbohydrates contributed to dental cavities and alcohol contributed to liver disease (15). When it came to meaty issues—fat and cholesterol as players in heart disease—the committee was a hot mess of disparity, disagreeing about whether the Dietary Goals’ meat-reducing recommendations were scientifically sound.
Charles Gluek, the expert in charge of the report’s fat section, announced: “There is no evidence, either observational or experimental, that conclusively demonstrates a causative relationship between dietary fat per se and human atherosclerotic disease.” Furthermore, he stated, “The benefits of a low-fat, low-saturated fat, low-cholesterol diet have never been adequately tested except in terms of reduction in plasma levels” (16). (For the record, the ASCN report only looked at different components of foods—not meat as a category.)
6. Wheat and the China Study
CLAIM: In explaining the dangers of “denialism” in scientific research, Davis cites the wheat and heart disease component of my 2010 critique of The China Study, a book by T. Colin Campbell. Davis states:
“A young schoolteacher … had basically looked at the raw data that Dr. Campbell collected and saw that one region of China ate lots of wheat and had a high amount of heart disease, which is counter to what was asserted in the book. … She did not look at any other factors that could have caused the relationship. Turns out this region of China ate very few vegetables and lots of meat” (page 142).
REALITY: These claims suggest Davis didn’t actually read the exchange! First, the wheat correlation came from pooling all of the China Study data (as published in the monograph Diet, Life-Style, and Mortality in Rural China), not from looking at a single county:

Second, as I explored in my follow-up post on wheat in the China Study, the relationship with heart disease stubbornly persisted even after adjusting for about 40 other variables in multiple regression models (contrary to Davis’s claim that “She did not look at any other factors that could have caused the relationship”). Those variables included:
- Animal food intake
- Animal protein intake
- Green vegetable intake
- Saturated fat intake
- Red meat consumption
- Total meat consumption
- Added animal fat
- DHA levels
- Folate levels
- Latitude (as a proxy for vitamin D)
- Five smoking and tobacco variables
Just to name a few!
Third, some of Campbell’s own peer-reviewed papers acknowledged (and corroborated) the China Study’s link between wheat and heart disease. In 1996, he co-authored a China Study-based paper that found wheat consumption was associated with lower levels of sex hormone-binding globulin, indicating greater insulin resistance (17). The paper stated:
“Significant differences in the diet of rural Chinese populations studied suggest that wheat consumption may promote higher insulin, higher triacylglycerol, and lower SHBG values. Such a profile is consistent with that commonly associated with obesity, dyslipidemia, diabetes, hypertension, and heart disease.”
And these examples are just the tip of the iceberg. Davis also makes some consistent errors when talking about other dietary movements. Which brings us to, drumroll please…
The Straw Men Cometh: Atkins, Weston A. Price, and Paleo Misrepresentations
Davis dedicates a number of impassioned pages to the Unholy Trinity of plant-based-diet rivals: the low-carbohydrate movement, the Weston A. Price Foundation, and the Paleo diet. He explains why these programs (which he stacks, collectively, under the “high protein” umbrella) are likely to make us sick, inflamed, miserable, and prematurely dead.
Alas, if Davis was hoping to win any friends from “the other side” with his book, this isn’t the best approach! The language is inflammatory: for low-carb, he refers to the “intellectual bankruptcy of the movement” (page 80), and he claims that Weston A. Price adherents “spew torrents of pseudoscientific mumbo jumbo that are simply baffling in their lack of resemblance to actual facts” (page 87). His treatment of each diet invokes both frank inaccuracies and easy-to-defeat straw man arguments, suggesting a lack of understanding (or lack of concern) with what they teach and espouse.
As a result, this section of the book is likely to make otherwise open minds slam irrevocably shut—alienating low-carbing, Paleo-dieting, or WAPF-following readers instead of inspiring them to hear a new perspective.
But don’t just take my word for it! Let’s hop on a safari through some specifics.
Low-Carbohydrate Diets
First, Davis first whisks readers through a brief tour of low-carbohydrate diets, emphasizing the unsavory: Dr. Robert Atkin’s controversial demise; Calories Don’t Count author Dr. Hermann Taller’s fraud charge; Dr. Irwin Stillman’s (of the Stillman Diet fame) death by heart attack. His descriptions imply that low-carb diets are akin to voluntary torture:
“People get so uninspired and bored, they unconsciously reduce the amount of food they eat” (page 81).
“Ask anyone who’s been on Atkins for a while: a slice of Pepperidge Farm white bread starts to look and smell like manna from heaven” (page 84).
“The Atkins empire lost steam in the 1980s, as more and more irritable, constipated, and nauseated former adherents literally became sick and tired of the boring diet and its consequences” (page 84).
He then proceeds to portray all lower-carbohydrate programs as being essentially the same:
“From Atkins sprung all sorts of diets, including Quick Weight Loss, the Scarsdale diet, Medifast, the Zone diet, the South Beach diet, the Sugar Busters diet, and many more. Their differences are superficial, and they cite insulin dumps from excess carbs as our biggest enemy. They refuse to … admit the long-term health consequences of their high-protein diets” (page 86).
These statements should set off some serious alarm bells! For one, Davis is conflating “low carbohydrate” with “high protein.” Those two terms definitely aren’t interchangeable, especially since some low-carb programs deliberately put a cap on protein intake (such as certain ketogenic diets or Jan Kwasniewski’s “Optimal Diet”), and some programs on his list aren’t even low carb (like Sugar Busters and the South Beach Diet, which might be better classified as low glycemic).
Two, calling the diets’ differences “superficial”—when they actually vary considerably in macronutrient ratios, rationale, and allowable foods—doesn’t do much to inspire trust in Davis’s expertise on the topic.
Equally concerning is Proteinaholic’s reliance on outdated review papers to challenge the safety of low-carb diets. In the book’s section on protein and early death, Davis references a 12-year-old paper with a doom-and-gloom message—even though far more current papers on the topic are available (18):
“In 2003, at the height of the Atkins craze, a couple of Australian scientists wrote a paper as a call to health professionals not to get taken in by the media frenzy. They warned that there was no good data to support the low-carb fad. To the contrary, the diet was linked to dangerous side effects’” (page 222).
Similarly, Davis cites an American Heart Association science advisory from 2001 as evidence that low-carb diets are risky, inadequately-studied leaps into the unknown (19):
“A 2001 review of the literature … noted that while high-protein, low-carb diets ‘may not be harmful for most healthy people for a short period of time, there are no long-term scientific studies that support their overall efficacy and safety’” (page 221).
Again, this paper was published almost 15 years ago—basically an eternity in the nutrition field.
Considering the sheer volume of low-carb research we’ve amassed since then, it seems odd that Davis doesn’t quote some of the more recent reviews available. We now have the results of a 44-month study on low-carbohydrate diets and diabetes, weight loss trials lasting up to two years, surveys of people who’ve been low-carbing for up to two decades, meta-analyses of weight loss and cardiovascular risk outcomes, and review papers that incorporate reams of shiny new data (20, 21, 22, 23, 24, 25, 26, 27).
The low-carb verdict? Nary an epidemic of exploding aortas, crumbling bones, or failing kidneys to be seen!
Davis also criticizes the Atkins diet by referencing a 15-year-old paper that he considers “an amazing review of the science behind popular diets” (page 84) (28). The review, he explains, stated that the Atkins diet is not only a bad choice for weight loss, but is also “accompanied by the kinds of side effects you usually find on the flip side of magazine ads for pharmaceutical drugs: constipation, bad breath, headache, nausea, and fatigue, among others” (page 84).
In nutrition, citing a 15-year-old review paper as evidence that low-carbing is bad would be like citing a 165-year-old map as evidence that North Dakota doesn’t exist. Sometimes the passage of time changes a thing or two!

What’s more, Davis doesn’t mention that this “amazing review” also warned against very low fat, plant-based diets—such as Dean Ornish’s—on account of nutrient inadequacy. The paper stated, “VLF [very low fat] diets are low in vitamins E, B12, and zinc because meat and fat intake is low.”
Ultimately, the only time more recent low-carb studies get a nod in Proteinaholic is when they don’t actually involve low-carb diets. For example, Davis discusses a 2013 meta-analysis that assigned people “low carbohydrate” scores, based on their relative intake of carbs and protein. The participants weren’t actually following low-carbohydrate diets—just chowing down on different shades of moderate carb and high carb within the Standard Western Diet spectrum—but Davis nonetheless relays, “Those who scored highest on the low-carb scale had a 31 percent increased chance of dying” (page 222) (29).
In the book’s chapter on protein and mortality, Davis cites a 2012 study involving 43,000 non-low-carbing women, which—through the wizardry of statistics and macronutrient relativism—concluded that “low-carb diets and high-protein diets both lead to increased cardiac and overall death” (page 225) (30). In fact, Davis explains, the study found that the “combination of low carb and high protein was the deadliest” (page 225).
Along with being blighted with that niggly problem of not actually studying people on low-carbohydrate diets, this paper was booed off the stage in editorial reactios. And for good reason! Canadian physician Yoni Freedhoff summed it up best:
“[The paper] bases all of its 15 years’ worth of conclusions on a single, solitary, and clearly inaccurate, baseline food frequency questionnaire; it didn’t control for clearly known dietary confounders; it found a miniscule absolute increase in risk; and the diet it reported on can’t even be fairly described as a low carbohydrate diet” (31).
Other critics submitted letters with titles like “Why did the BMJ publish such a biased article?” and aired qualms about the study’s methodology, execution, and conclusions (32).
Ironically, Davis frequently (and rightfully) laments the fact that many so-called “low fat” studies aren’t actually low fat, and that the poor definition obscures the benefits such diets can bring. Why not apply that same logic to low carbohydrate research?
Lastly and most tragically, there probably are some critique-worthy elements of low-carbohydrate diets that Davis could’ve focused on—like the long-term effects on cortisol, thyroid, fertility, gut ecology, and other issues that have popped up anecdotally but haven’t been the focus of organized studies yet. By parroting the anti-low-carb rhetoric promulgated by its rival communities (especially those of the vegan variety), Davis misses a chance to deepen the dialogue, and his treatment of low-carb diets comes off as cliché rather than persuasive.
The Weston A. Price Foundation
The next misrepresentation victim is the Weston A. Price Foundation (WAPF), which Davis calls “one of the strangest organizations I have ever seen” (page 87). It’s odd that Davis files them under the high-protein label, seeing as the foundation has specifically stated “most of us do well on a diet that has 10-15 percent of calories as protein,” asserted that “Twenty percent of calories as protein is the maximum,” and warned that “a diet too high in protein … can rapidly deplete vitamin A,” a nutrient the organization famously reveres (33). Nonetheless, let’s assess some of Davis’s other criticisms against the WAPF to see if they hold water.
Price’s Research
 The WAPF is rooted in the research of Weston A. Price—an American dentist who traveled the globe in search of healthy, non-Westernized populations, scouring their diets for clues about optimal nutrition. He published his findings in his 1939 opus, Nutrition and Physical Degeneration, which distilled the recurring themes of those indigenous diets: an absence of refined sugar, refined flour, canned products, and vegetable oils, and a lusciously high intake of fat-soluble vitamins from animal foods (especially organ meats, insects, fish roe, and dairy from spring-grass-guzzling cows).
The WAPF is rooted in the research of Weston A. Price—an American dentist who traveled the globe in search of healthy, non-Westernized populations, scouring their diets for clues about optimal nutrition. He published his findings in his 1939 opus, Nutrition and Physical Degeneration, which distilled the recurring themes of those indigenous diets: an absence of refined sugar, refined flour, canned products, and vegetable oils, and a lusciously high intake of fat-soluble vitamins from animal foods (especially organ meats, insects, fish roe, and dairy from spring-grass-guzzling cows).
Describing Price’s legacy, Davis states:
“… understand that his research was purely observational. Rather than providing the ‘scientific proof’ that WAPF acolytes claim, his wanderings and observations can provide questions for further research, but no answers” (page 89).
“Price did make many keen observations, but he did not engage in any kind of scientific evaluation [in terms of setting up experiments]” (page 90).
Actually, Price did conduct experiments to test his nutritional hypotheses, equipping him with clinical data to support his ethnographic findings (34, 35). Along with experiments on lab animals, he treated his most cavity-prone human patients with cod liver oil or butter oil—testing whether the addition of “activators” (later identified as fat-soluble vitamins A, D, and K2) would boost calcium metabolism, heal troubled teeth, and rev up immunity. (These were the same common-denominator nutrients abundant in the indigenous diets Price encountered in his travels.)
As described in his 1932 paper, “Control of Dental Caries and Some Associated Degenerative Processes Through Reinforcement of the Diet with Special Activators,” the fat-soluble vitamin experiments were nothing to sneeze at (35):
- One woman with dry mouth (xerostomia) and debilitating arthritis was also given cod liver oil as an experiment: “The treatment has been continuous during these years and she has been practically free from arthritis.”
- In a group of 78 patients with cavities, the most severe cases downed a mixture of high-vitamin butter oil and high-vitamin cod liver oil. Before the experiment, they averaged about eight cavities per person; after one year of treatment, they averaged less than 1.5 cavities per person.
- One 14-year-old patient with 17 cavities was treated with cod liver oil for a year: “During this year, no new cavities had formed and, in addition, as shown in the illustrations, there was a marked improvement in the density of the teeth.”


- A group of 56 patients—comprised of teenagers, boarding school attendees, and pregnant women—were either given cod liver oil (the experimental group) or given nothing (the control group). “These studies revealed that those in each group that were receiving [cod liver oil] treatment showed marked improvement.” Indeed! The post-experiment scores:
- The cod-liver-oiling teenagers boasted a whopping zero cavities, compared to an average of 5.5 cavities per mouth for the control group.
- The boarding schoolers’ experimental group had zero cavities, compared to an average of 8.5 cavities for the control group.
- The pregnant women taking cod liver oil had one cavity in total, compared to nine for the control group.
- In a study of 200 people, 100 were left as controls and 100 were treated with “activator” vitamin capsules: “The number of cavities per person in the group not receiving the capsules was for all ages ten times that which occurred in the group receiving the capsules.” That difference was even more striking in teenagers: “in the twenty persons not receiving additional vitamins in capsule form, the total number of cavities was 143, and in the group of twenty receiving the additional vitamins, there were three cavities in the entire group.”
In other words, Price was far from a passive observer! His clinical experiments confirmed that the fat-soluble vitamins abundant in the diets of healthy, non-Westernized populations were key for immunity, skeletal structure, and maintaining a stellar set of pearly whites.
WAPF on Vegetarianism
Next up, Davis comments on the Weston A. Price Foundation’s stance on vegetarianism, noting that Price himself admired the health of certain vegetarian populations (like the north Indian Pathans, who he called ‘the most perfect people in India’). Davis writes: “Interestingly, Price was not antivegetarian, a fact that would surprise his so-called followers were they to take his work seriously” (page 90).
This actually shouldn’t come as a surprise. While the WAPF certainly warns against pure vegan diets, the foundation isn’t necessarily anti-vegetarian. Their website includes a “vegetarian tour” that states:
“The Foundation believes that strict vegetarianism (veganism) is detrimental to human health. Vegetarianism that includes eggs and raw (unpasteurized) dairy products, organic vegetables and fruits, properly prepared whole grains, legumes, and nuts, and excludes unfermented soy products and processed foods, can be a healthy option for some people.”
WAPF on Grains and Legumes
Likewise, Davis notes that Price was “enamored” with the grain-eating Gaelics, Swiss, and the Neur tribe of Africa, and that his dietary recommendations—as conveyed in a letter to his nieces and nephews—included eating whole-grain wheat, rye, and oats, including cereal and breads (page 90). Davis comments,
“It is therefore very difficult for me to understand how current foundation members extrapolate Price’s observation to a philosophy that consists of … avoiding grains and legumes like the plague” (page 90).
 Again, this statement reveals Davis’s lack of familiarity with what the WAPF espouses. Far from avoiding these foods “like the plague,” the organization is a vocal proponent of many wondrously grainy and legumey items—one of the main dividing lines between them and by-the-book Paleo dieters. The WAPF’s official dietary guidelines include “whole grains, legumes and nuts that have been prepared by soaking, sprouting or sour leavening.” Likewise, items in the “best” category of their shopping guide include:
Again, this statement reveals Davis’s lack of familiarity with what the WAPF espouses. Far from avoiding these foods “like the plague,” the organization is a vocal proponent of many wondrously grainy and legumey items—one of the main dividing lines between them and by-the-book Paleo dieters. The WAPF’s official dietary guidelines include “whole grains, legumes and nuts that have been prepared by soaking, sprouting or sour leavening.” Likewise, items in the “best” category of their shopping guide include:
- Organic dried beans
- Lentils
- Whole grain rice
- Whole grains (except bulgur)
- Whole grain breakfast cereals that must be cooked
- Wildcrafted wild rice
- Organic popcorn (to pop at home)
- Sourdough or sprouted breads made from freshly ground, organic, whole grain flour
- Freshly ground and soaked organic whole grain flours
- Freshly ground organic sprouted/dehydrated grains
- Sourdough or sprouted crackers made from freshly ground, organic, whole grain flour
If the WAPF is anti-grain and legumes, this seems like an odd way to go about showing it!
WAPF on Plant Foods
Lastly, Davis accuses Sally Fallon, president of the WAPF, of crafting “prose worthy of George Orwell’s Big Brother” in her interpretation of Price’s diet recommendations (pages 90-91).
To kick things off, Davis tries to make the case that Price was mostly a plant-food pusher—exalting all things grain, legume, and vegetable as dietary centerpieces:
“Dr. Price wrote an enlightening letter to his nieces and nephews, detailing how they should eat to stay healthy, and how they should feed their children. Here’s a direct quote: ‘The basic foods should be the entire grains such as whole wheat, rye or oats, whole wheat and rye breads wheat and oat cereals, oat-cake, dairy products, including milk and cheese, which should be used liberally, and marine foods.’ He also advised his young family members to consume vegetables and especially lentils” (page 90).
Davis then cites a passage from Fallon’s article “Interpreting the Work of Dr. Weston A. Price,” which he calls “a masterpiece of cherry-picking … [insisting] that Price’s real recommendations were the opposite of those he himself penned” (pages 90-91). As evidence of this backwardness, Davis pulls the following quote from Fallon:
“‘… as Price perceived so clearly, the only way for humans … to properly nourish themselves is to eat mostly nutrient-dense foods; and the emerging science of biochemistry confirmed the dietary habits of primitive peoples by revealing just which foods best meet these requirements—all of them animal foods, and not necessarily steak or chicken but seafood, and milk products and organ meats from animals raised on mineral-rich soil” (page 91).
Speaking of picking cherries, Proteinaholic just served up a few fruity bowls itself! First, Davis’s quote from Price leaves out the great emphasis placed on seafood. Immediately following the excerpt Davis relayed from Price’s letter, Price had written:
“All marine or sea foods, both fresh and salt water, are high in minerals and constitute one of the very best foods you could eat. Canned fish such as sardines, tuna or salmon are all excellent; also the fresh seafood such as oysters, halibut, haddock, etc.” (36).
“There are only a few foods that would give you your fat-soluble vitamins. These are the fish products, including practically all fresh water and salt water foods, milk, cheese and butter made from cows that have been on a rapidly growing green young wheat” (36).
Last time I checked, fish and dairy don’t exactly grow on trees!
What’s more, Price wrote this particular letter in 1934—right after he’d visited the isolated Swiss and Gaelics (who ate abundant grains and minimal land meat), but before he’d extended his travels to the Melanesians, the Polynesians, multiple African tribes, the Australian Aborigines, the Torres Strait Islanders, the New Zealand Maori, and the Peruvian Indians, all of whom influenced his nutritional worldview (and scooted “organ meats” and other animal foods higher up on his dietary hierarchy). The letter, then, hardly reflects the conclusions he reached from the totality of his research.
Second, it’s ironic that Davis accuses Fallon of misrepresenting Price’s work, when Proteinaholic quite blatantly misrepresents hers. Out of Fallon’s entire 8,300-word article, Davis chose the only paragraph that—plucked out of context—seems to endorse a carnivorous diet and gloss over Price’s comments on plant foods. Elsewhere in the article, Fallon liberally quotes Price’s pro-plant, moderate-protein sentiments:
“‘There is no objection to having the children fill up on bulky foods such as potatoes and vegetables, if the daily mineral and vitamin requirements have been satisfied first,’ he advised his nieces and nephews.”
“Price did not advocate a high-protein diet. ‘The protein requirement can be provided each day in one egg or a piece of meat equivalent to the bulk of one egg a day,’ was his Depression-era advice.”
“Price … did not advise his patients to avoid high-carb foods like fruits, whole grains or root vegetables. These he considered an important adjunct to the diet. He was particularly enamored of poi, the fermented taro preparation of the South Sea Islanders.”
“… not all of the groups Price studied ate diets rich in animal foods. All of the ones who were healthy, however, did eat at least some animal products. Many of these subsisted largely on animal products while some subsisted largely on plant products. Among those who were healthy and ate a small percentage of their calories as animal products, they selected very nutrient-dense products such as whole insects and frogs, shellfish, and so on.”
“The diet Price used with his patients … was not devoid of plant foods or very low in carbohydrates. The Weston A Price Foundation and Sally Fallon’s book Nourishing Traditions do not recommend specific carbohydrate and fat guidelines.”
In all, Davis appears to be repeating the common misconceptions about the WAPF—especially ones ever-rattling through the vegan and vegetarian communities—without having fact-checked them for validity.
The Paleo Diet
No plant-based diet book would be complete without taking a few brass-knuckle swings at Paleo, and in this sense, Proteinaholic fulfills its duty!
Actually, Davis is much kinder to the Paleo movement than many critics are. He praises the “societal benefit” that comes from getting people to “[think] about their food in a critical way, no longer willing to unquestionably swallow industrial food,” and comments on the legitimate value of boycotting low-nutrient, industrially processed fare—a Paleo upside he calls “not insignificant” (page 94).

But that’s where the extended olive branch ends. Davis first dishes up some very valid criticisms of the diet, which Paleo adherents themselves might even agree with:
“… the original notion of a Paleo diet has now morphed into a giant industry, consisting of a confusing mess of products. Paleo bread, cookies, and protein bars are all touted as functionally equivalent to what prehistoric man may have consumed” (page 95).
“… consider how unlikely it would be for actual Paleo man to have such an abundant supply of meat to be able to eat it three times a day” (page 95).
“… most diets view legumes as the enemy, even though every population study that has investigated the claim has correlated high legume consumption with health and longevity” (page 95).
Although a deeper discussion of these points is beyond the scope of this critique, the Reader’s Digest version is: nailed it!
Davis is correct: Paleo has birthed its own “food industry,” including a deluge of processed products that probably aren’t much healthier than their non-Paleo counterparts. Multiple-times-per-day meat feasts have very little historical precedent. And indeed, the only way to link legumes with obesity and chronic disease is to ignore a glut of direct research and operate entirely in theory. (Though to be fair, we do have some evidence that autoimmune conditions and certain gut disorders could be aggravated by components of legumes (37, 38, 39).)
These are conversations already rumbling through the Paleo community, and Davis is wise to point them out.
Alas, Davis also fires some shots that radically miss the mark. In critiquing the concept of ancestral eating, he hones in on the Paleo Diet™ promoted by Loren Cordain—a very specific (and literally trademarked) brand of Paleo that doesn’t really represent the movement as a whole. (Cordain espouses a higher-protein, lower-fat program that nixes all dairy, starchy foods, and added salt—far from universal Paleo tenets.)
To commence the debunking, Davis addresses Cordain’s assumption that humans are genetically hardwired to eat “lots of meat” simply because Paleo man did the same (page 97). To crush this argument, Davis whips out two counterpoints:
“First off, prehistoric man … ate what was available because otherwise he starved. He made decisions on food based not on optimal health, but rather survival” (page 97).
“Second, there’s no such thing as ‘the’ Paleo diet; patterns of eating varied tremendously from region to region and season to season. The idea that there existed one specific Paleo diet is pure fiction” (page 97).
 Point one is perfectly legit (and is a major reason why the concept of “reenactment Paleo” is hardly embraced anywhere outside of Flintstones reruns). Most thought-leaders in the Paleo movement treat early human diets as a starting place rather than a final destination.
Point one is perfectly legit (and is a major reason why the concept of “reenactment Paleo” is hardly embraced anywhere outside of Flintstones reruns). Most thought-leaders in the Paleo movement treat early human diets as a starting place rather than a final destination.
But that second point? It’s curious Davis fires this as anti-Paleo ammo, since it’s a belief the Paleo community already shares. In fact, to support his “no specific Paleo diet” claim, Davis cites a paper written by none other than Boyd Eaton and Melvin Konner—co-authors of the 1989 book The Paleolithic Prescription, and veritable grandfathers of the Paleo movement (40). Their paper acknowledges a wide range of animal food intakes among early humans (stating that Paleolithic diets were “based on as much as 80 per cent or as little as 20 per cent meat” by weight), but their work hardly undermines Cordain’s promotion of omnivory (40).
Davis also comments on Cordain’s use of the Ethnographic Atlas—a sprawling database of over 1200 societies, published in 1967 by George Peter Murphy—to estimate the diets of hunter-gatherer tribes (41). Davis says that the atlas “found a lot of animal bones and what appeared to be hunting implements,” leading Cordain to conclude that “ancient man ate lots of meat” (page 97). Davis continues:
“What’s laughable about this, of course, is that bones and stones are precisely the sorts of material that might last long enough to be found by researchers tens of centuries later. The remnants of the nuts, seeds, berries, leaves, roots, and stems that composed the lion’s share of the diet would have been long gone, and therefore unable to offer their evidence to the atlas makers” (page 97-98).
Here, Davis appears to confuse the Ethnographic Atlas with a collection of archaeological digs. Not the case! The atlas didn’t rely on ancient remains; it curated centuries of direct observations of still-existent societies—some dating back before the 1500s—regarding subsistence activities (hunting, fishing, gathering, animal husbandry, and agriculture), family structure, monogamy versus polygamy, settlement patterns, the taboo-ness of cousin marriages, dwelling types, religious beliefs, game-playing habits, and a variety of other fascinating variables that anthropologists and behavioral scientists go gaga over.
Cordain used the atlas to identify pure hunter-gatherer societies (the ones with 100% dependence on fishing, hunting, and gathering), and calculated their plant versus animal food ratios from there (42). His belief was that modern hunter-gatherers might give us a clue or three about the diet of early humans. No bones or stones involved!
 After knocking down the Ethnographic Atlas straw man, Davis suggests some better ways to determine what our ancestors ate. He cites one example of a mostly-plant-noshing hominin—the two-million-year-old Austalopithecus sediba, whose fossilized dental plaque was analyzed for carbon isotopes—as evidence that “ancient man was a heavy plant consumer” (43, 44, 45).
After knocking down the Ethnographic Atlas straw man, Davis suggests some better ways to determine what our ancestors ate. He cites one example of a mostly-plant-noshing hominin—the two-million-year-old Austalopithecus sediba, whose fossilized dental plaque was analyzed for carbon isotopes—as evidence that “ancient man was a heavy plant consumer” (43, 44, 45).
While our friend Au. Sediba is definitely a fascinating specimen, it hardly supports the claim that early humans were mostly vegetarian. As one of Davis’s own references explains, Au. Sediba’s preferred menu “differed in fundamental ways from the diet of all other australopithecines and later hominins studied so far,” being characterized by C3 foods (fruits, leaves, nuts, forest-dwelling creatures, and other forest fare) rather than C4 foods (grassland plants and the animals that graze on them) (46). In fact, a number of other early hominin fossils reveal more omnivorous inclinations—not just based on tool and skeletal remains, but also on nitrogen isotopes, which can gauge a creature’s average protein intake and estimate its level of animal food consumption (47, 48, 49, 50).
And the questionable anthropological conclusions don’t end there! In discussing the Neanderthals, Davis offers this nugget:
“… no matter what region of the world is studied, analysis of Neanderthal teeth proves that these humans ate mostly plants, including legumes” (page 98).
The ‘evidence’ in question comes from a 2011 paper, “Microfossils in calculus demonstrate consumption of plants and cooked foods in Neanderthal diets”—which, to riff off of Inigo Montoya, does not mean what he thinks it means (51). This paper discussed the fantastic diversity of cooked starch and legume consumption among Neanderthals, in addition to their meat-full menus—a far cry from painting them as eating “mostly plants.” In fact, the paper concluded with a solid vote in favor of omnivory:
“Overall, these data suggest that Neanderthals were capable of complex food-gathering behaviors that included both hunting of large game animals and the harvesting and processing of plant foods” (51).
What’s more, nearly every other analysis of the Neanderthal diet—whether gleaned from isotopes, tool remains, fecal fossils, or dental wear and calculus—suggests they were far from plant-based in their munching habits. For example:
- “The high proportion of very large herbivores … in Neanderthal’s diet … suggests that Neanderthals could not acquire these prey through scavenging. They probably had to hunt for proboscideans and rhinoceros” (52).
- “… on the basis of available Sr, Ba, and Ca contents of plants, the results indicate that the percentage of plants in the Neanderthal’s diet must have been close to zero … the calculation shows that bovids (except reindeer) represent the greatest percentage of consumed meat (58%), followed by horses/rhinoceros (22%), reindeer (13%), and mammoths (7%)” (53).
- “We found that the Jonzac Neanderthal had isotopic values consistent with a diet in which the main protein sources were large herbivores, particularly bovids and horses” (54).
- “The isotope evidence overwhelmingly points to the Neanderthals behaving as top-level carnivores, obtaining almost all of their dietary protein from animal sources” (55).
- “Analysis of five sediment samples from different occupation floors suggests that Neanderthals predominantly consumed meat, as indicated by high coprostanol proportions” (56).
All that being said, Davis’s Neanderthal citation does cramp the style of some Paleo beliefs, as it shows starchy grains and legumes were being eaten—albeit probably not in staple-level quantities—far earlier than previous timelines suggested. As mentioned earlier, the legume issue really deserves more objective treatment by the low-carbohydrate and Paleo communities: despite hypothetical concerns about their lectins and phytates, legumes have consistently been shown to improve glycemic control, reduce heart disease risk factors, improve inflammation (including CRP levels), reduce lipid peroxidation, and generally improve metabolic health in a variety of controlled trials (57, 58, 59).
In fact, Proteinaholic’s argument against the Paleo diet might have been more convincing if Davis spent time expounding the legume issue instead of misrepresenting ethnographic and anthropological data!
Cherry-Picked Deaths
As a final nail in the coffin for animal-protein-rich cuisines, Davis brings up the early or disease-shrouded deaths of Robert Atkins, Stephen Byrnes (of the Weston A. Price Foundation), Weston A. Price himself, and a handful of others who seemed to perish before their time. He states, “I just find it odd that these leaders of a dietary movement are dying from the diseases they claim their diets prevent” (page 91).
Although it’s awfully tempting to get swayed by anecdotes, similar (and equally fruitless) arguments could be made against veganism as well. Consider:
- Jay Dinshah, the founder and former president of the American Vegan Society, died of a heart attack at age 66—after being a vegetarian from birth and a vegan since his early 20s (60).
- T.C. Fry, an early raw vegan pioneer, died of a coronary embolism when he was around 70 years old—and additional blood clots in his legs were found during his autopsy (61).
- Vihara Youkta, a 30-year raw vegan and wife of raw food pioneer Viktoras Kulvinskas, died of bowel cancer at the age of 58 (62, 63).
- Harvey Milstein, leader of the vegan “Natural Hygiene” movement in Davis’s hometown of Houston, died of colon cancer in his late 60s—after 23 years as a raw vegan (64, 65).
And of course, some low-carb advocates have lived long, juicy, starchless lives—such as Wolfgang Lutz, author of Life Without Bread, who lived to be 97 (66). Ultimately, calling out individual leaders’ longevity (or lack thereof) tells us little about the healthfulness of their diet on a larger scale.
Does Animal Protein Cause Weight Gain?
One of the most eyebrow-raising, counterintuitive claims in Proteinaholic is that animal protein promotes weight gain, and is at least partly responsible for the obesity epidemic seizing the Western world. (News, no doubt, to the legions of body-builders downing whey protein shakes and chicken breasts while chiseling away their body fat!)
The immediate problem with this argument is that we’re swimming in research showing that protein is the most satiating macronutrient, boasts a significant thermogenic (heat-producing) effect, and is incredibly inefficient to store as fat (67, 68, 69). So, the idea that it uniquely promotes weight gain could be summed up with a quote from Mr. Carl Sagan: “Extraordinary claims require extraordinary evidence.” We would need some pretty impressive data to topple our prevailing understanding of protein’s effects on appetite and weight regulation. Can Davis deliver?

Before tackling Davis’s theory on why protein causes weight gain, let’s take a look at his attempts to disassemble the existing notions of why it causes weight loss. (Public Service Announcement: for this section of Proteinaholic, it’s supremely important to fact-check any claims against their cited references, because they often don’t match up.)
First, Davis targets the idea that high-protein diets increase metabolism via thermogenesis—which, he explains, “basically means that the body has to expend energy to process protein” (page 181). While admitting there’s some validity there, he quickly argues that the impact is too small to matter:
“Studies have shown that basal metabolic rate increases when eating protein. … The fact is, however, that this effect is tiny, maybe a 1 to 2 percent increase, which is about 20 calories” (page 181).
To support this statement, Davis cites a paper comparing 24-hour energy expenditure among diets that swapped out dietary fat for animal protein (pork), vegetable protein (soy), or extra carbs (70). All three diets had the same number of calories, fiber, and fat.
Lo and behold, a “1 to 2 percent increase [in metabolic rate]” from eating protein is a misunderstanding of the study’s results. The researchers found that basal metabolic rate (BMR) was 2.5% higher for the animal protein diet compared to the plant protein diet. That’s right: this study actually showed that animal protein boosts metabolism more than plant protein!
But that’s just the difference between the two protein types. When compared with the carby diet and baseline diet, the effect of protein-enriched diets was even more dramatic. Animal protein from pork resulted in a BMR that was 4.5% higher than the carb-rich diet and 5.0% higher than the baseline diet. (For soy protein, average BMR was 2% higher than the carb-rich diet and 2.4% higher than the baseline diet.)
So now, it’s not a matter of 20 calories a day, but—in the case of animal protein—almost 114 extra calories getting guzzled up by folks’ metabolic furnaces every 24 hours. This comes out to about 41,500 calories a year, or almost 12 pounds of potential body fat. Not so trivial anymore, eh?
What’s more, the study also found that animal protein cranked up diet-induced thermogenesis (3.5% higher than the vegetable protein diet, 5.5% higher than the carby diet, and 3.8% higher than baseline). Sleeping energy expenditure, daytime energy expenditure, and 24-hour energy expenditure were all highest with the animal protein diet as well.
And fascinatingly, out of all the diets, the one filled with vegetable protein resulted in the lowest level of 24-hour spontaneous physical activity. That includes stuff like fidgeting, toe-tapping, shifting around while sitting, standing up, pacing across the room, and other little actions that your mom probably told you to knock off when you were a kid. Collectively, these activities actually seem to protect against fat gain on a long-term basis (71, 72, 73, 74).
For some reason, spontaneous physical activity was 3.5% lower than baseline when folks were eating the vegetable protein diet—compared to the animal protein diet, which was 1.6% higher than baseline. (The high-carb diet was slightly under baseline as well.)
How come? It’s basically a mystery, but the authors offered the following guess:
“Twenty-four–hour spontaneous physical activity tended to be lower with the soy diet than with the pork and carbohydrate diets, indicating that consumption of soy protein may lower physical activity. The reason for this is unknown; however, a difference in amino acid-specific effects on sympathetic activity is a possible explanation.”

But we’re just getting started! A bit later, Davis makes another questionable claim: “the science does not show that protein has a dramatic independent effect on eating behavior” (page 182).
To back up this statement, he cites a 2012 study that prodded deeper into the “protein leverage hypothesis”—that is, the idea that our bodies regulate protein intake more strongly than total energy intake (75). If we eat foods with low ratio of protein to fat and carbohydrate, the theory posits that we’ll just keep eating until we reach the threshold of protein that makes our appetites go, “Aha! Enough eating has been done” (76, 77).
While this study didn’t find that a low protein ratio encourages overeating, per se, it did find that a higher protein ratio absolutely curbs appetite. Something that could surely be called a “dramatic independent effect on eating behavior,” which is what Davis implies isn’t the case.
In this study, participants spontaneously lowered their energy intake when their diets had a higher proportion of protein. We’re talking a drop in over 580 calories per day, in fact, when comparing an ad libitum 30% protein diet to a 15% protein diet, and a reduction of over 500 calories per day when comparing a 30% protein diet to a 5% protein diet (75).

The researchers noted:
“Appetite scores were similar between the conditions, despite the intervention-induced lower energy intake in the high-protein condition, which indicates that subjects were similarly satiated and satisfied by the diets, including less eating with a high-protein diet.”
To his credit, Davis does acknowledge that protein has a uniquely satiating effect in some studies, but doesn’t think those findings carry over into our day-to-day lives. He claims, “In the real world … food choices do not seem to be governed independently by protein” (page 182).
To support this assertion, he discusses a paper called “A satiety index of common foods,” noting that the winner of the Satiation Prize was an undeniably carby tuber (78):
“In one study, researchers had test participants eat various different foods in equal energy amounts. They tested fullness after the meal and the amount of food eaten at the next meal. The higher-carbohydrate potato actually had the highest satiety index” (page 182).
Although it’s true that potatoes ranked the highest (a satiety-index score of 323, with 100 being “white bread equivalent”), it’s likely due to their preparation method more than anything inherently appetite-slaying about carbohydrates.
In this experiment, russet potatoes were boiled and refrigerated overnight (at 4°C) before consumption—a fabulous way to create retrograded resistant starch, which significantly lowers the potato’s glycemic index, makes a hefty chunk of it indigestible, and independently boosts satiety (79, 80, 81).
That said, a number of protein-rich foods also dominated the charts. For example, ling fish—the highest-protein item on the list—beat out every non-potato plant food measured (all fruits, legumes, and grains), with a satiety score of 225. Beef (a score of 176) ranked more satiating than lentils (133), brown rice (132), white rice (138), whole-meal bread (157), bananas (118), grapes (162), muesli (100), baked beans (168), popcorn (154), peanuts (84), all breakfast cereals except porridge, and all bakery products. Eggs and cheese had higher satiety scores than bananas, most cereals, and other starchy foods—but since they’re also quite high in fat, their scores might be expected to lag behind leaner protein sources (82).
This study also contradicts another of Davis’s statements, where he claims protein only seems more satiating in studies because it’s being compared to faux-food concoctions of refined sugars and starches:
“Studies comparing protein to carbs for satiety give protein the edge in blunting hunger, but these studies use isolated carbs, not fruits and veggies. … We know that eating pure sugar can make you hungry by affecting blood glucose levels. By not testing protein directly against fruit and vegetables, which have the sugars bound to fiber and therefore control hunger better, these satiety studies make protein look better than it really is” (page 181) (83).
Again, the “Satiety Index” study pitted fiber-rich carbohydrates (including whole fruit) against protein sources, and still found protein to be a strong satiation contender. We’ve got a number of other experiments in the same vein, too, with similar results—using items like meat casserole versus vegetarian casserole, or comparing meat and dairy products to carbs that were “primarily vegetables, fruits, breads, rice, and pasta” (84, 85).

“Dare I eat a peach?”
Even more problematic, Davis’s explanation for why high-protein foods (and diets in general) are more satiating involves a few logical blunders. He writes:
“… satiating [is] a funny word for what really happens. If you eat a very low-carb diet, your body runs out of its primary form of energy: carbs. To stay alive, your body … will start burning fat for fuel, with chemicals called ketones created as a by-product. Ketones can make you feel ill. Complaints of nausea and abdominal discomfort are common on these diets and may be the reason people end up eating fewer calories” (page 181).
What’s wrong with this picture? Let us count the ways!
- Once again, Davis is conflating low-carbohydrate diets with high-protein diets. They aren’t the same thing! Most studies showing a satiating effect of protein use moderate to high levels of carbohydrates, making it almost impossible to sling people into ketosis—and therefore nullifying the rationale Davis presents for protein’s tendency to reduce appetite (75, 84, 86).
- Consuming too much protein tends to prevent ketone production, because the excess protein gets converted into glucose (via gluconeogenesis) (87). So, Davis’s ketones-make-people-queasy explanation would only be valid in the case of high fat, low carb, low-to-moderate protein diets—not simply high protein diets.
- A number of mechanisms have been identified explaining why protein is satiating, and none have to do with ketones. For instance, peptide YY, ghrelin, gastric emptying speed, glucagon-like peptide-1, insulin, and cholecystokinin all seem involved in a lovely appetite-suppressing tango for those who feast on protein (88, 89, 90, 91, 92).
Volumetrics: When Size Really Does Matter
With so many Satiation Points scored in protein’s favor, we’d need some pretty compelling evidence to make the case that—on the whole—protein encourages weight gain. Is there some sort of counterintuitive, long-term effect of protein on appetite regulation? On body fat storage? On hormones associated with satiation? Could a cod filet that curbs hunger one day have a fattening boomerang effect later on?
According to Davis, the explanation is actually much simpler. His chief hypothesis for the question of “Why does protein cause weight gain?” boils down to one thing: volumetrics (page 186).
Volumetrics is a concept based on the energy density of foods—that is, calorie content relative to volume. The theory goes that bulky, low-energy foods (vegetables, fruit, brothy soups, and the like) will trigger “stretch receptors” in the stomach, signalling fullness to the brain. On the flip side, low-volume, high-energy foods (like oils, sugar, and anything that’s come within 10 feet of Paula Deen) won’t create physical fullness until we’ve already gorged ourselves on more fuel than we need (pages 186-187) (93, 94, 95).
Davis illustrates this idea with some basic math:
“… if you eat a giant 280 gram slice of watermelon, due to the fiber and water, you get only 85 calories. A 280 gram piece of chicken delivers almost six times the calories (480). If you could actually consume 280 grams of olive oil (20 tablespoons, in case you’re crazy), you’d take in a whopping 2,380 calories” (page 187).
Although volumetrics seems logical enough (and does have some science-approved relevance in weight management), it falls apart as an argument against protein. If we look at the actual energy density values of different foods (measured as calories per 100 grams), we’ll quickly see that the highest-protein animal products are actually similar (or lower!) in energy density than many whole, plant-based items (96):
- Chicken breast has similar energy density to garbanzo beans
- White fish (like flounder and sole) has lower energy density than cooked lentils, brown rice, and sweet potatoes
- Pork lunch meat and cooked eggs have similar energy density to pinto beans
- Baked salmon has lower energy density than avocados (and similar density to olives)
- Egg whites have similar energy density to peaches and berries
- Oysters have lower energy density than potatoes and bananas

The only way to indict animal foods on the volumetrics front is to focus on the fattiest fare (like butter and salami and cheese)—but then the argument isn’t about protein, but fat. And that’s an issue that certainly isn’t exclusive to the animal kingdom. Nuts, seeds, coconut meat, and plant oils all dominate the density list—peanut butter is on par with bacon!—and nowhere does Davis accuse these foods of driving the Westernized world’s expanding waistlines. (In fact, Proteinaholic’s recipe section liberally features walnuts, almonds, pistachios, hempseed, sunflower seeds, cashews, tahini, coconut milk, coconut oil, olive oil, and even nondairy margarines like Earth Balance—all of which, per the volumetrics theory, should be more fattening than lean animal protein (pages 289-324).)
To bolster the idea that high-volume, low-energy-density, plant-based diets promote easy weight loss, Davis cites the Waianae Diet Study—a trial that placed native Hawaiians on a menu resembling their pre-Westernized traditional diets for 21 days. The participants could dine on unlimited amounts of taro, poi, sweet potato, yams, breadfruit, geens, fruit, and seaweed, along with up to 198 grams of fish and chicken per day. (The cuisine averaged a spartan 12% fat and 11% protein, the rest coming from carbs (97).)
As Davis explains,
“Despite the lack of limits, [the participants] ended up eating fewer calories while showing significant improvements in their cardiometabolic profile. They also lost an average of 10.8 pounds over the three weeks” (page 188).
The Waianae Diet Study is absolutely interesting, but not for its value as low-protein evidence. A similar study was conducted in Australia the 1980s: a group of urban-dwelling Aborigines spent seven weeks reverting to a traditional hunter-gatherer diet filled with kangaroo meat, turtle, fresh-water fish, birds, yams, honey, figs, and veggies (98). Due to the high proportion of lean wild game, the traditional diets were incredibly rich in protein—an average of 54% of calories—and lower in carbohydrate (33% of calories), with the remaining 13% squeezed from fat.
As with the Waianae dieters, the Aborigines saw fabulous improvements in their health. They lost an average of 17.5 pounds over the course of seven weeks, and across the board, their metabolic problems (all participants were diabetic at the outset) either radically improved or vanished into thin, Down-Under air.
From a macronutrient perspective, the only thing the Waianae study and Aboriginal study had in common was a very low percentage of fat. Protein didn’t seem to make a lick of difference!
What About Observational Studies?
Nestled in a series of weak protein-causes-weight-gain arguments is something legitimately noteworthy: the results of the European Prospective Investigation into Cancer and Nutrition (EPIC) study.
We’ll delve into this project in more depth later on, but on the obesity front, one particular finding stood out. Davis writes:
“The EPIC study researchers … followed hundreds of thousands of people over several years and found that, contrary to popular belief, the more animal protein people ate, the more likely they were to become obese” (page 184) (99, 100).
And not just any animal protein, either: according to one analysis, chicken was the prime correlate for weight gain over time (101).
Putting aside the fact that observational studies can’t take us all the way to the “causation” finish line (and assuming the poultry-in-question wasn’t of the Kentucky Fried variety), the chicken conundrum is an intriguing one.
Why? Poultry is generally crowned with a health halo in the public’s mind—that is, the perception of being healthy, which leads health-conscious folks to pile more of it on their plates. Whereas red meat tends to carry a hefty not-good-for-you stigma, bringing with it some statistical baggage (people who eat more red meat are more likely to smoke, be sedentary, drink too much, and care less about the prospect of an early grave), the same can’t be said for poultry. That makes it far less likely that lifestyle confounders were behind the poultry and weight-gain relationship.
So, could anything explain this correlation other than something inherently fattening about bird meat?
Actually, yes! One fascinating possibility comes from a recent analysis of chicken meat. Due to modern farming methods, the fat content of broiler chickens has been steadily increasing for decades—to the point where now, store-bought chicken actually contains over twice as many calories from fat as from protein, and 25% less protein that it did in the days of yore (102, 103).
Based on these updated calculations, a plumped-up chicken eaten in 2004 would boast almost 20% more calories than a similar bird consumed in 1991.

Why does this matter? Because the EPIC researchers estimated nutritional content of foods based on older, pre-existing chemistry reports, rather than directly analyzing each forkful of food that entered participants’ mouths (104).
If the EPIC researchers were using outdated nutrient values for chicken, they may have underestimated the energy provided from poultry. That would skew calculations for people’s calorie intake and muddy any attempts to control for total energy in the study’s statistical models. As a result, poultry-noshers would’ve looked like they were eating fewer calories than they really were—giving the illusion of chicken correlating with higher BMI and weight gain independent of calorie intake. Wham, math!
(And in case you’re wondering: yes, this could potentially mean the energy density of chicken discussed earlier in this critique is totally wrong! Welcome to the ever-revising world of nutrition.)
A second (but equally important) issue is the way food intake was determined in the EPIC study. As one of Davis’s cited reports explains, folks’ dietary patterns were measured only once during the entire many-years-long study—at baseline, when they first enrolled as participants (101). There were no updates collected afterwards to see if people’s diets had changed and if they were still eating the same quantities of chicken over time.
In studies with less happy outcomes for vegetarians and vegans, Davis pounces on this only-at-baseline measurement method for its obvious weaknesses. For instance, when listing off some findings from the Adventist Health Study 2, he hedges the unimpressive results like so:
“There are a couple of caveats to this study. For one thing, participants’ diets were assessed only once, at the start of the study, and never reassessed. We simply don’t know if participants changed their diets during the study, which obviously would have major implications for the results” (page 229).
This criticism could be applied pretty much verbatim to the EPIC study. In fact, another comment in the EPIC paper suggests the participants’ diet measurements may, indeed, have been misleading—not just from changing as the years rolled on, but also from being poorly representative of what folks were eating before they enrolled in the study. As the researchers explained (emphasis mine):
“… when subjects with previous illness and those likely to misreport their energy intake at baseline were excluded from the analyses, the association of weight gain with poultry was attenuated and the strongest association was observed for processed meat. This suggests that this result may be driven mainly by subjects with previous illness or weight-loss attempts that lead to diet intervention, as well as those who misreported their dietary intakes.”
So, is chicken a propeller of weight gain or a useful adjunct for weight loss? The fattier, omega-6-rich nutrition profile of chicken compared to birds of yesteryear is certainly a concern, but from a purely evidential standpoint, it doesn’t seem to be fattening up humankind.
Does Animal Protein Contribute to Cancer?
The idea that animal protein spurs cancer growth is one of the most vociferous battle cries of the plant-based-diet crowd, having first gained traction after T. Colin Campbell’s The China Study hit the stands. Proteinaholic continues the tradition!
Davis (bless his heart) avoids citing the China Study to support an animal protein-cancer connection, but he does present a torrent of mechanisms to argue that protein-rich animal foods contribute—in various ways—to that loathesome “C” word. Some of these mechanisms include:
- Heterocyclic amines (HCAs)
- Heme iron and N-nitroso compounds
- IGF-1
- A reduction in protective bacteria
- Methionine
- Acidosis
- Neu5Gc
- Hormone plasma levels
- Slaughterhouse chemicals
Out of all the protein-centric sections of his book, this one probably offers the most legitimate precautions for meat consumers. Alas, very few of Davis’s cited mechanisms indict animal protein itself: many are dependent on the type of meat, the way it’s raised and handled, the way it’s cooked, and what other foods accompany it at mealtime—all of which can be altered without going full-throttle vegan.
So, which of these mechanisms might be true concerns? Let’s take a gander!
 Heterocyclic Amines (HCAs): These carcinogenic compounds form when muscle meat (like beef, chicken, pork, or fish) is heated at high temperatures or over an open flame (105). Although the link between HCAs and cancer is pretty solid in animal studies, the doses used are typically between 500,000 and three million times higher than what humans ingest from food (106). And more importantly, any legitimate risk can be obliterated simply by avoiding super-high-temperature cooking. Some spices and marinades can also mitigate HCA formation—black pepper, rosemary extract, grape seed extract, extra virgin olive oil, onion, or garlic, for example (107, 108, 109, 110).
Heterocyclic Amines (HCAs): These carcinogenic compounds form when muscle meat (like beef, chicken, pork, or fish) is heated at high temperatures or over an open flame (105). Although the link between HCAs and cancer is pretty solid in animal studies, the doses used are typically between 500,000 and three million times higher than what humans ingest from food (106). And more importantly, any legitimate risk can be obliterated simply by avoiding super-high-temperature cooking. Some spices and marinades can also mitigate HCA formation—black pepper, rosemary extract, grape seed extract, extra virgin olive oil, onion, or garlic, for example (107, 108, 109, 110).
Plus, the high-heat issue is hardly exclusive to animal protein. Some cooking methods create carcinogens in plant foods, too—like acrylamide that forms in potatoes and other asparagine-rich starches (111, 112, 113). (Funnily enough, just as certain plant components can reduce HCA formation in meat, certain animal food components—namely the amino acid glycine, rich in bone broth and connective tissue—can reduce acrylamide formation in plants (114).)
Heme Iron and N-Nitroso Compounds: Heme iron is probably one of the most flamboyantly flapping red flags on the meat and cancer front. A compelling number of studies show that heme iron contributes to the formation of N-nitroso compounds and toxic aldehydes, both of which can play roles in initiating colorectal cancer (115).
However, the effects of heme iron are supremely context-dependent! Consuming chlorophyll-rich foods (like leafy greens and other plant matter) along with iron-rich animal foods effectively nullifies the effects of heme iron (116). The reason? Chlorophyll is so structurally similar to heme that it actually blocks its metabolism in the intestinal tract, stymieing the formation of toxic metabolites.
Bottom line? Consuming a high-red-meat diet with scant plant matter could be bad news for colon health. The problem can be mitigated, though, by eating liberally from the vegetable world.
Insulin-Like Growth Factor 1 (IGF-1): This growth factor is critical for helping produce tissue and synthesize new cellular DNA, but too-high levels have been implicated as a cancer risk-raiser—especially of the breast, prostate, and colon. Davis asserts that restricting animal protein can coax IGF-1 into falling, hypothetically slashing cancer risk. He also states that eating animal products results in higher circulating IGF-1 (both from internal production and from IGF-1 entering our bodies from foods—especially hormone-treated dairy).
The reality? “It’s complicated.” For one, the link between IGF-1 and cancer isn’t fully conclusive. Two, IGF-1 is influenced by a huge number of factors: along with protein (both animal and plant!), it’s been connected to dietary fat, high-glycemic carbohydrates, caloric excess, obesity, and other decidedly non-proteinful variables (117, 118, 119). Three, regardless of the effect of any specific foods on IGF-1 levels, other diet and lifestyle habits—such as intermittent fasting and maintaining a healthy body weight—can help suppress IGF-1 and keep levels in a healthy range, without requiring a commitment to low-protein veganism.
Reduction in Protective Bacteria: Although it only makes a cameo appearance in this book, the issue of gut bacteria might actually be a big deal for long-term low-carbers, as some experts have proposed. Davis describes one study in which a low-carb diet led to “decreases in key protective bacteria” and “significant reduction in butyrate production,” and mentions another study where a low-carb diet (the legit kind—5% of calories from carbohydrates) produced higher levels of harmful metabolites (page 191) (120, 121).

The only problem? The microbiome-disturbing effect doesn’t seem to be a consequence of eating too much protein, but eating too little plant matter—especially the fermentable carbohydrates that feed beneficial gut microbes. Another easy fix that doesn’t require abandoning animal foods.
Methionine: Davis references a stack of longevity research showing that restricting methionine, an amino acid, leads to longer lifespans and lower cancer risk—at least in rodents. (As for our own species, “Researchers are continuing to test the hypothesis that methionine restriction may increase life span in humans” (page 198).) Since methionine is richest in muscle meat, eggs, dairy, and fish (with nuts and seeds getting honorable mention), it seems to be a smoking gun for the animal protein-cancer link.
But there’s another side to the story! Additional research suggests that amping up intake of glycine—another amino acid abundant in animal foods, found in skin and connective tissue and bone—can have the same life-extending effects as methionine restriction (122). Of course, those are the animal parts we usually discard these days, but it doesn’t have to be that way! The issue of methionine-glycine balance makes a pretty strong case for eating nose-to-tail rather than consuming exclusively muscle meat, but hardly stands as an argument to avoid animal protein categorically.
Acidosis: A handful of times in Proteinaholic, Davis brings up the controversial concept of acidosis to undermine the wisdom of eating animal protein. I say “controversial” because the concept has, by the power vested in the internet, become a parody of itself: there’s a difference between “acidosis” (a process that calls upon the body’s compensatory mechanisms to buffer acidity) and “acidaemia” (a blood pH of less than 7.35, which can get very lethal very quickly), but the terms tend to be clumsily and chronically interchanged (123).
Despite cyber-claims to the contrary, low blood pH (acidaemia) won’t happen just by eating too many animal products. Acidosis, though? It seems to be a thing. And the net acid load of the diet—that is, the balance between acid-forming components (like sulfuric acid) and base-forming components (like bicarbonate)—may indeed have relevance to human health.
Prior to the book’s cancer section, Davis explains that “When our body becomes too acidic, a state known as metabolic acidosis, our tissues become inflamed” (page 150). As a potential cancer mechanism, he proposes that chronic acidosis wreaks havoc at a cellular level in ways that promote malignant formations, though he doesn’t get any more specific than that (page 198).
Let’s suspend disbelief for a minute and assume that a chronic acid load may, indeed, kick off the cancer process. This is where the targeted indictment of animal foods falls apart! Several of Davis’s references note that along with animal protein, cereal grains are rich in sulfur-containing amino acids that generate sulfate, a “major determinant of the daily acid load” (124). One reference states that both “animal products and cereals [are] more acidogenic than fruits and vegetables” (125).
And left out of the discussion entirely is the fact that some animal-based foods, like gelatin, are low in sulfur-containing amino acids. Along with the methionine/glycine issue, that may help explain why “nose-to-tail” eating has been a much more successful model of omnivory than our modern fixation on muscle meat (126).
Neu5Gc: Neu5Gc is a sialic acid molecule found in red meat, and it’s shown up in small amounts in cancerous tumors. Although humans can’t produce Neu5Gc on our own (due to a many-moons-ago genetic mutation), we can incorporate it into our tissues and generate anti-Neu5Gc antibodies (127). Some researchers speculate the immune response to these antibodies can fire up chronic inflammation, contributing to cancer and other diseases as a result.
Although it’s a fascinating theory, there’s a light-year-long leap between our current patchy evidence and any solid disease links! As a recent paper described, feeding people large quantities of Neu5Gc didn’t cause their levels to rise from baseline—suggesting our understanding of how this molecule gets incorporated into tissue still has a long way to go (128). That same paper theorized that early childhood exposure to Neu5Gc in cow milk or vaccines, transfer of Neu5Gc from mother to baby, or a preexisting immune response may be required for Neu5Gc to make its way into human cells. In other words, it’s dastardliness is context dependent, and likely only affects a portion of the population.
So, to worry or not to worry: that is the question! While Neu5Gc may end up being relevant, we can’t know until the literature starts veering towards much more conclusive grounds. This one’s a big fat “maybe” on the Concerned Omnivore list.
Hormone Plasma Levels: Davis discusses the potential for animal protein to bump up levels of estrogen (and other hormones) in the body, possibly boosting the risk of hormone-sensitive cancers like prostate cancer and breast cancer.
 Although the link between nutrition, hormone levels, and certain cancers is probably real, animal protein per se might be an unwitting whipping boy here. In studies, the direct relationship between meat and dairy and hormone-related cancers has been pretty dodgy (129, 130, 131). Dairy pops up as a correlate with prostate cancer fairly often, but the mechanism appears more calcium-related than a consequence of too much protein (132). And although there’s still quite a bit of debate whirling around the subject, hormones used in some commercial farming practices (like rBGH) could play a role—stacking some points in favor of choosing organically raised animal products over conventional items (133).
Although the link between nutrition, hormone levels, and certain cancers is probably real, animal protein per se might be an unwitting whipping boy here. In studies, the direct relationship between meat and dairy and hormone-related cancers has been pretty dodgy (129, 130, 131). Dairy pops up as a correlate with prostate cancer fairly often, but the mechanism appears more calcium-related than a consequence of too much protein (132). And although there’s still quite a bit of debate whirling around the subject, hormones used in some commercial farming practices (like rBGH) could play a role—stacking some points in favor of choosing organically raised animal products over conventional items (133).
Slaughterhouse Chemicals: Davis notes a well-established pattern where slaughterhouse and processing-plant employees have higher rates of certain cancers (one, sorry dudes, being that of the penis) (134). Exposure to chemicals and other carcinogens involved in meat processing is the very likely culprit!
However, Davis offers no evidence that these workplace toxins actually hitch a ride on the meat and end up on consumers’ plates—making this more of an “occupational hazard” concern than a dietary one. And speaking of meat processing…
Welcome to the Jungle: Do Cancer Rates Among Immigrants Indict Meat?
Early in Proteinaholic, Davis whips out a fascinating reference to a 1907 New York Times article, which—despite being over a century old—boasts a headline that could’ve been plucked straight from a modern-day newsfeed: “Cancer Increasing Among Meat Eaters” (135).
The article reported on a seven-year study of Chicago immigrants, showing that recent arrivals from Germany, Ireland, Slavonia, and Scandinavia were experiencing veritable explosions in their cancer rates. Although Davis doesn’t quote the exact figures, the original source shows they’re pretty stunning: during the seven-year period, cancer mortality among those immigrant groups was over 24 times higher than for native Chicagoans—a difference of 178 cancer deaths among the Chicago-born versus 4,463 cancer deaths for the newcomers. This, despite the fact that immigrants comprised only about a third of Chicago’s total population!
As Davis explains,
“[The article] suggested that part of the problem was the way immigrants were switching from their traditional plant-based diets to meat-rich fare once they began to establish themselves in America. The lead researcher was quoted as saying, ‘There cannot be the slightest question that the great increase in cancer among the foreign-born over the prevalence of that disease in their native countries is due to the increased consumption of animal foods’” (pages 63-64).
 In other words, cancer seemed go hog wild (pork pun totally intended) as soon as the immigrants indulged in America’s meaty abundance. The two immigrant groups that purportedly didn’t rev up their meat intake—the Italians and Chinese—maintained their long-standing good health.
In other words, cancer seemed go hog wild (pork pun totally intended) as soon as the immigrants indulged in America’s meaty abundance. The two immigrant groups that purportedly didn’t rev up their meat intake—the Italians and Chinese—maintained their long-standing good health.
The reason this study is so valuable? Unlike today, the early 1900s still featured plenty of pasture-raised animal products as the norm—so things like hormone injections, sketchy feedlot practices, antibiotic use, and other confounders that obscure animal food studies today weren’t part of the equation. That makes a pretty clear argument for something being inherently hazardous with meat… right?
Actually, there’s more to the story! For one, the passage Davis quotes has a conspicuous six-word omission: the rest of the sentence from the article reads (emphasis mine):
“There cannot be the slightest question that the great increase in cancer among the foreign-born … is due to the increased consumption of animal foods, particularly those derived from diseased animals.“
And by “diseased,” we aren’t talking a few sniffles and a cough. Immigrants were feasting chiefly on meat from animals that had been condemned ante-mortem (before slaughter) for tuberculosis, actinomycetosis, and cancer, and that had been raised on objectionable diets of “wet malt or distillery slop.” After the animals’ diseased organs and body parts were lopped off, about 87% of the condemned meat passed into the market for purchase, and was “largely consumed by the foreign poor.” Bon appetite?
A longer discussion of Chicago’s cancer conundrum appeared in volume 20 of The Chicago Clinic in 1907 (136). Here, the same researcher noted that, according to his investigations, wet-malt-fed meat had higher toxicity to living tissue when compared to “properly pastured” meat. On top of that, samples of breast milk, urine, and feces from immigrants eating condemned meat products had greater toxicity than the same secretions from people eating fresh, pastured meat.
And diseased animals weren’t the only issue here, either. According to the study, the nationalities with higher cancer rates “consumed large quantities of canned, preserved, dried, and pickled meats, [and] sausages”—largely because fresh meat was more pricey (and the cheaper processed meats earned some Budget Brownie Points as a result). Apparently, the nationalities with the highest cancer rates were “immense consumers of meat products which, if unpreserved, would be intolerable even to themselves.”
In a nutshell, immigrants weren’t just eating more meat: they were specifically eating more heavily processed meat—from animals literally bursting with tumors, infected organs, and other malformed bits—while simultaneously eating less of the fresh, expensive pastured meat also available at the time.
As further evidence this was probably a quality-over-quantity issue, it was noted that Chicago natives—who were hardly known for eating a plant-based diet at the turn of the last century—had “about the lowest death rate from cancer of any people in the world.” The main difference between them and immigrants? A proclivity for fresh meat versus the cheaper canned, salted, pickled, or cured goods (or “bads,” as the case may be).
And lastly, there may be a simpler explanation for the cancer explosion as well. Bear in mind, this study was published in 1907—one year after Upton Sinclair’s famous exposé, The Jungle, blew open the dirty secrets of Chicago’s meatpacking district, leaving a trail of gaping jaws and dry-heaving stomachs in its wake. The Jungle described the atrocious conditions of meatpacking workers: poisoned rats dying atop flesh piles and getting processed into sausage; men’s fingers devoured to nubs by pickling acid; workers tumbling into open vats and getting rendered, in the company of swine, into lard. (Not surprisingly, The Jungle caused a public uproar so momentous that the government ended up passing the Federal Meat Inspection Act and the Pure Food and Drug Act to appease its distraught citizens—a story for another day!)

Chicago meat packing industry, circa 1905: Swift & Co.’s Packing House: cutting up hogs, removing hams and shoulders. Via Library of Congress.
Here’s why this matters. The vast majority of meatpackers at the turn of the 19th century were immigrants—and in particular, the very groups with the highest rates of cancer. The Germans and Irish, whose early-1900s cancer death rate was “the highest in the world” (according to the New York Times article that reported on this study), dominated Chicago’s meatpacking industry until the year 1900 (137).
And as we touched upon earlier, it just so happens that meat industry workers, regardless of diet, suffer from wildly disproportionate rates of cancer—including lung cancer, pharynx cancer, esophageal cancer, colon cancer, bladder cancer, kidney cancer, bone cancer, leukemia, and lymphoma (138, 139, 140, 141, 142, 143, 144, 145, 146, 147). Exposure to smoke, incomplete combustion products, fumes from meatpacking materials, carcinogenic viruses (such as the bovine leukemia virus and bovine papilloma virus), polycyclic aromatic hydrocarbons, nitrosamines, and various other occupational hazards could very well have driven the excessive cancer rates among certain immigrant groups (148, 149).
So, was this Chicagoan cancer trend a product of increased meat consumption, or were other factors hiding behind that worrisome correlation? All signs point to the latter!
Are Vegans and Vegetarians Healthier than Meat Eaters?
Throughout Proteinaholic, Davis cites observational studies suggesting that vegans (and to some extent, vegetarians) are healthier and longer-lived than those who partake in all manner of animal protein. Although observational studies are notoriously correlative, incapable of ever proving cause and effect, they’re sometimes the best thing we’ve got when long-term controlled trials are improbable or impossible. (As fantastic as it’d be to kidnap two twins at birth, raise them in environmentally identical bubbles, feed one an omnivorous diet and the other a vegan diet, and see what happens over the course of the next 80 years, it might be hard to slide that design by an ethics committee.)
So, do these veg-versus-omni studies prove that the no-meat crowd, all else being equal, enjoys superior health and longer lifespans than their omnivorous counterparts?
EPIC-Oxford Study
One of Davis’s most well-trodden references is the European Prospective Investigation into Cancer and Nutrition (EPIC)—namely the Oxford branch, which recruited tens of thousands vegetarians and vegans, as well as relatively health-aware meat eaters.
Before we get to the study’s findings, let’s look at how Davis characterizes EPIC-Oxford. On multiple occasions, he implies that the meat-eating group had an unfair advantage over the vegetarians and vegans due to their abnormally health-aware status. In his own words:
“The Oxford branch of the EPIC study looked at a population of meat eaters that was healthier than average (partly because their meat intake was much lower than that of the general population) and compared them to a rather unhealthy group of vegetarians” (page 159).
And again, later:
“The Oxford branch … [compared] unhealthy vegetarians to healthy meat eaters. To remind you: the vegetarians showed B12 deficiencies and ate paltry amounts of fiber for people who were supposed to be eating veggies. The meat eaters consumed a relatively low average of 64 grams of meat per day” (pages 169-170).
Because of this supposedly uneven playing field, Davis pooh-poohs one of the study’s less favorable findings as a fluke: rates of colon cancer were actually higher among vegetarians than in meat eaters (page 207). Davis rationalizes this stat on the basis of the vegetarians’ fiber intake (or lack thereof) and concludes they were eating health-damaging processed foods.
Fiber-wise:
“So why did EPIC-Oxford show increased risk? … One of the protective effects of being vegetarian/vegan is presumably eating more plants and therefore more fiber. However, this group of vegetarians didn’t eat nearly the amount of fiber you would expect for plant eaters” (page 208).
And junk-food-wise:
“Other studies on this group show that they don’t take B12 and many don’t take calcium. Not the healthiest group of vegetarians. We can only conclude that while they were not eating meat, they must have been eating processed junk food” (page 208).
This weaves together a lot of assumptions—some of which aren’t supported by the data, and some of which are patently illogical.
For one, a closer look at what the different dietary groups were eating shows the vegans (and vegetarians) were still chowing down on significantly more fiber (in grams per day) than the recruited meat eaters. Per Davis’s logic, that fiber boost should’ve conferred more colon cancer protection and kept the vegetarians’ rates lower than the omnivores’.

That being said, just a few pages earlier in the book, Davis actually cast doubt on the fiber-colon cancer connection entirely—citing a major study that failed to christen fiber as Colon Cancer Protector Extraordinaire:
“A 2005 meta-analysis of 13 large-scale prospective studies following 725,000 men … found that fiber intake is only weakly correlated with decreased rates of colorectal cancer. It may be that avoiding the meat protein is a bigger deal than eating lots of produce” (page 202).
Secondly, Davis’s implication that the vegetarians were somehow less healthy relative to the omnivore group is highly misleading. Along with the fiber issue, meat eaters appeared less health conscious on a number of fronts.
Their fruit and vegetable intake was lower (150):


Graphs from “Lessons for vegetarians and vegans from the EPIC-Oxford study.”
Their alcohol intake was higher (151):

They had a higher percentage of heavy smokers:
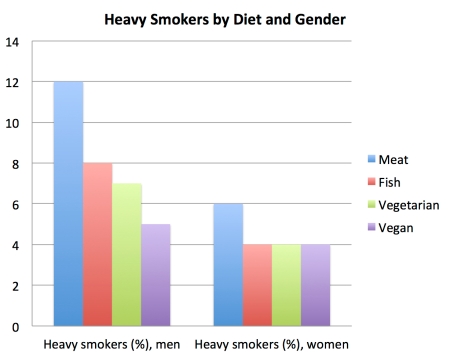
They had a lower percentage of “highly active” people:

So, the vegans still had the advantage in this study—just by a smaller margin than we usually see. And frankly, the fact that the EPIC-Oxford omnivores were healthier than Standard-Western-Diet omnivores should be considered a huge plus! Typically, studies of vegans versus omnivores are caked with confounding that’s hard to scrape off, even with the most intensive statistical scrubbing. Meat-avoiders are dramatically more likely to exercise, drink less, smoke less, be more educated, eat more fruit and vegetables, and express other distinct differences relative to their omni counterparts—all of which stack the deck in their favor in terms of health outcomes (152).
Although scientists have ways to mathematically adjust for those legs-up, the accuracy of the adjustments depends on the accuracy of the original data. And as any researcher knows, getting people to correctly report their food intake, exercise habits, and alcohol consumption is almost as easy as getting them to run a marathon in stilettos. In fact, food frequency questionnaires—a staple for gauging people’s diets in observational studies—are shockingly unreliable, and have been repeatedly criticized for their limitations (153, 154).
So, studies that avoid these initial confounders by using equally matched omnivores and vegetarian groups are serious gems! They can isolate the effects of animal food intake far more effectively than studies requiring elaborate statistical footwork. In that sense, Davis should be praising the slightly-more-level playing field in the EPIC-Oxford project, rather than portraying it as some sort of liability.
Davis’s second assertion—about the vegan group not taking vitamin B12 or calcium and thus presuming “they must have been eating processed junk food”—is also highly questionable. For one, Davis spends part of Proteinaholic expounding why a low calcium intake among vegans and vegetarians shouldn’t be a problem, claiming that animal protein is what raises calcium requirements due to its acidifying effect on the body (pages 267-268). He states that the “bottom line is that there is ample calcium in fruits and vegetables,” and proclaims, “Eat your greens and you don’t have to worry about your bones”—nary an advisory to be seen about calcium supplements (page 268).
In addition, Davis doesn’t offer any citations for his claim that “Other studies on this group show that they don’t take B12” (another purported indication that the meatless were careless about their health), but a scour of the existing literature shows this might be a bit misleading:
- Early EPIC-Oxford publications only measured total B12 intake from food and beverages, with the specific caveat that supplements weren’t included in the calculations (150, 155).
- Later publications found that almost five time as many vegans and vegetarians supplemented with B12 compared to omnivores—a difference of 19% versus 4%, respectively (156). And while anything less than a 100% supplementation rate might seem disconcerting for a group whose diet fundamentally eschews natural B12 sources, it’s not necessarily an indication of health-unconsciousness. Seventh-day Adventist vegan and vegetarian ministers, renowned for their commitment to healthy living, only supplemented B12 at a rate of 12% when surveyed during the same time period as the Oxford vegetarians (157).
Plus, at the time the EPIC-Oxford supplement data was collected, a number of prominent vegan health figures were pretty lackadaisical on the supplement-promoting front. Dr. John McDougall, for instance, was only recommending B12 supplements for people who’d been vegan for three years or longer (as well as pregnant or nursing women) (158).
Likewise, many vegans may have been operating under the assumption that fortified foods (or even unwashed, B12-producing-bacteria-laden plant foods) would provide all the B12 they needed. Vegan dietitian Jack Norris, RD, explains what seems to be a still-enduring problem:
“Despite the overwhelming evidence that vegans without a reliable source of vitamin B12 are likely harming their health, some vegan advocates still believe that ‘plant foods provide all the nutrients necessary for optimal health,’ and do not address vitamin B12 when promoting the vegan diet. Other advocates acknowledge the need for B12, but only as an afterthought. And still others emphasize that humans need only small amounts of B12 and that it can be stored in the body for years” (159).
In other words, low B12 supplementation rates may have had less to do with the vegans’ and vegetarians’ commitment to staying healthy, and more to do with the educational climate of the time.
So, the portrayal of the EPIC-Oxford vegans as a processed-food-guzzling, supplement-indifferent group really isn’t backed by the evidence! All indications point to the meatless participants being the most health-savvy of the bunch.
With all that in mind, let’s take a look at some of the Oxford findings Davis relays as evidence for vegan and vegetarians’ superior health. First, Davis states:
“The EPIC-Oxford data, while probably underestimating the benefits of a vegetarian diet and downplaying the risks of a high-protein diet due to previously mentioned issues with subject selection, nevertheless was able to find mortality differences. The vegans in the study … suffered less mortality from heart disease, cancer, and all causes” (pages 225-226) (160).
Curiously, Davis supports this statement with a paper from 1999 that discusses the Oxford Vegetarian Study, not the EPIC-Oxford study—two horses of a figurative different color, despite their shared geography.
And it turns out, the results from EPIC-Oxford painted a much different picture! A 2009 analysis found that “mortality from circulatory diseases and all causes is not significantly different between vegetarians and meat eaters” (161). (Vascular disease and all-cause mortality rates were actually slightly higher (though not statistically-significantly so) among vegetarians compared to meat eaters.)
Piggybacking off his previous assertion, Davis cites another paper (involving the Oxford Vegetarian Study and Health Food Shopper Study—not EPIC-Oxford) as evidence that even small forays into meat eating spell trouble or health (162):
“Interestingly, the control group of meat eaters in this study ate meat infrequently, around once a week and yet still had higher risk of premature mortality compared with vegetarians” (page 226).
This is an odd conclusion to draw from a paper that found vegetarians and meat eaters were essentially on par with each other mortality-wise, and that avoiding meat had little to do with the health benefits of vegetarianism! Verbatim:
“British vegetarians have low mortality compared with the general population. Their death rates are similar to those of comparable non-vegetarians, suggesting that much of this benefit may be attributed to non-dietary lifestyle factors such as a low prevalence of smoking and a generally high socio-economic status, or to aspects of the diet other than the avoidance of meat and fish.”
It doesn’t get much clearer than that!
Diving back into the calcium topic, Davis gives a selective interpretation of an important finding. He implies that vegans are at no greater risk of fractures than omnivores, stating:
“The EPIC study found that vegans who ate a minimal 525 milligrams of calcium daily (the equivalent of one Tums tablet) had the same fracture rates as their meat-eating counterparts” (page 268) (163).
Omitted from this discussion is the fact that almost half of the participating vegans (44.5%) ate less than 525 milligrams of calcium per day. And when the full group of animal-food abstainers was analyzed, their fracture rate was somewhat alarming. Even after adjusting for age, smoking, alcohol intake, BMI, exercise, hormone replacement therapy usage, calorie intake, and calcium intake, the vegans had a higher risk of fracture than any other dietary group:

Although calcium intake seemed to be the wizard behind the fracture curtain, the researchers also suggested the fracture-proneness of the vegan group could have been due to—wait for it!—their low animal protein intake:
“Although the lower mean calcium intake among the vegans in this study seems to be the most likely explanation for their higher fracture rate other dietary factors need to be considered. Cross-sectional data from the EPIC-Oxford study showed that the vegans have the lowest mean intake of protein. … Increasing protein intake raises the circulating level of insulin-like growth factor-1, which promotes osteoblast formation and bone growth.”
Oxford Vegetarian Study and Health Food Shoppers Study
Apart from being accidentally cited under the guise of EPIC-Oxford (and a brief allusion by name on page 225), the Oxford Vegetarian Study and Health Food Shoppers Study remain conspicuously undiscussed as far as their findings go. And for the sake of preserving Proteinaholic’s thesis, that’s probably a good thing: they both cast doubt on the idea that avoiding animal protein makes for a healthier human body!
A recent combined analysis of the Oxford Vegetarian Study and the EPIC-Oxford cohort found no overarching mortality benefit from nixing all animal foods (164). And although vegetarians and vegans as a collective group seemed to have some advantage, it disappeared for vegans when they were analyzed as a separate category. According to the researchers:
“Separating the vegetarians and vegans for the 6 most common causes of death did not reveal any statistically significant differences in mortality between vegans and regular meat eaters.”
In fact, although the numbers didn’t reach statistical significance, vegans actually had the highest rates of all-cause mortality, respiratory diseases, cerebrovascular disease (including stroke), and malignant cancer:


As far as the Health Food Shoppers Study went, the results were equally underwhelming for the meatless. Compared to ominvores, the study’s vegetarians had slightly higher total mortality, and significantly higher rates of breast cancer among the ladyfolk (165):

(This study didn’t distinguish vegans from vegetarians, though, so we can’t speak for those who eschewed everything from the animal kingdom.)
Nurses Health Study and Health Professionals Study
Beyond EPIC-Oxford, Davis cites a litany of other observational studies that seem to cheerlead for Team Veganism. Another heavy hitter is the Nurse’s Health Study (and Health Professionals Study), which followed female and male health professionals, respectively, in prospective-cohort fashion.
Davis claims these studies provide evidence that “more plants and fewer animals in the diet equals increased life expectancy” (page 230). A 2008 analysis, he explains, found that a “prudent eating” pattern slashed all-cause mortality by 17% and cut heart disease deaths by 28% (166). He writes,
“How did they define ‘prudent eating’? High fruit and vegetable consumption and low red and processed meat consumption” (page 230).
Once again, some game-changing details are left out! In the researchers’ own words, “high prudent pattern scores represented high intakes of vegetables, fruit, legumes, fish, poultry, and whole grains” (167). “High intakes of fish and poultry” is a far cry from “fewer animals in the diet.”
The Seven Countries Study
Another go-to reference for meat critics (Davis included!) is the Seven Countries Study—a sprawling epidemiological project spearheaded by the infamous Ancel Keys. Describing one Seven Countries analysis, Davis writes:
“A 2000 update found a direct correlation between saturated fat, smoking, and low vitamin C intake and all-cause mortality. … Of course, saturated fat mainly comes tied with animal protein” (page 224-225).
The update in question did, indeed, find that saturated fat, smoking, and low vitamin C all contributed (at least in a mathematical sense) to total mortality rates (168). But the assumption that saturated fat was a proxy for animal protein—and that if protein had been measured in this study, it would’ve ended up on the killer list too—is a pretty big stretch. Another Seven Countries analysis measured all the macronutrients and found that, while total mortality was correlated with saturated fat intake, it was wholly unrelated to the amount of protein people were eating (169).
And as luck would have it, the Seven Countries data repeatedly coughed up glowing endorsements for one of nature’s richest sources of animal protein: seafood! A few findings that—not surprisingly—didn’t make it into the pages of Proteinaholic:
- In Zutphen, the Netherlands, men who ate at least 30 grams of fish per day had a 50% lower risk of dying from heart disease than men who didn’t eat fish at all (170).
- Fish-eating men (at least 20 grams per day) also had a 50% lower risk of stroke than men who either didn’t consistently eat fish, or who didn’t eat fish at all (171).
- Among the elderly, fish consumers had a significantly lower rate of cognitive decline compared to non-consumers (172).
- Fish—especially fattier varieties rich in omega-3—was associated with a 34% reduction in coronary heart disease mortality in three different European countries (173).
Adventists
Also docked in the meat-free evidence queue are the Adventist Health Studies, conducted on Adventist adherents—many of whom opt for a vegetarian or vegan diet as part of their religious practice. Davis calls them a “wonderful natural experiment,” noting that the cohort as a whole is spectacularly health-conscious, and participants differ chiefly in their level of animal food inclusion (104):
“They do not drink or smoke, they exercise moderately, and they strive to eat healthy. … [But] there’s a lot of dietary variation among Adventists even as their lifestyles are quite similar in all other respects. They comprise a mix of meat eaters, fish eaters, vegetarians who consume dairy, and a relatively large group of vegans” (page 147).
From there, Davis serves up a platter of citations that seem to support lower meat consumption: a 1988 Adventist analysis connecting meat with all-cause mortality, heart disease, and diabetes; a 1999 paper showing vegetarians were getting significantly less colon, prostate, and bladder cancer than meat eaters; an analysis of over 71,000 people revealing that those who slashed down on animal protein had lower body mass (page 228, 212, 185) (174, 175, 176). On the surface, these trends look pretty incriminating for those who dare flirt with omnivory.
But as usual, that’s only one piece of the puzzle. Where Davis goes astray is in the assumption that Adventist omnivores and their vegan and vegetarian brethren differ only in animal food intake. As it turns out, this isn’t the case!
One analysis found that compared to Adventist meat eaters, the cohort’s vegetarians drank less coffee, ate fewer donuts, and ate more tomatoes, legumes, nuts, and fruit (175). In fact, the researchers concluded that “among Seventh-day Adventists, vegetarians are healthier than nonvegetarians but this cannot be ascribed only to the absence of meat.”
And it doesn’t end there! Another paper found that Adventist vegans watched less TV, got more sleep, drank less alcohol, and were less likely to smoke—all indicators of an overall more-health-conscious lifestyle (177):
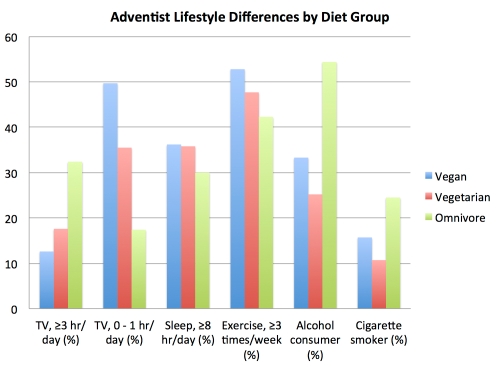
So right from the get-go, it’s clear that the Adventists don’t have virtually homogenous lifestyles, distinguished only by a proclivity (or lack thereof) for flesh and dairy foods. As with the general population, they’re burdened with the confounder of meat consumption correlating with riskier health behaviors.
And despite an initial advantage, not all of the Adventist Health Study reports showed vegans taking the health lead. For instance, one important finding is tucked into a study from 2013—a 5.8-year follow up for the Adventist Health Study 2 (178). First, here’s Davis’s take on this paper:
“When vegans, lacto-ovo-vegetarians, pesco-vegetarians, and semivegetarians were combined into one group, they had a 12 percent lower risk of mortality than the nonvegetarian Adventists. … Vegans by themselves had a 15 percent lower risk of death, but it did not quite reach statistical significance” (page 228).
What’s missing from this picture? Something fishy! When each diet group was analyzed separately, seafood-eaters actually came out ahead, beating the vegans for all-cause mortality, ischemic heart disease, and cardiovascular disease protection:
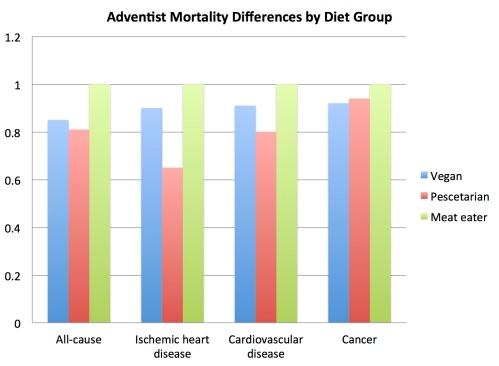
Another vote, it seems, for creatures of the sea.
So, what can we conclude about the Adventists? Despite the misconception that vegans, omnivores, and everyone between follows a similarly squeaky-clean lifestyle within this community, the data says otherwise. And even a face-value interpretation of its most recent findings suggest that eating seafood is superior to total animal food abstinence, as far as health outcomes go.
What About the Mechanisms?
Davis wisely avoids ending his “less meat, longer life” argument on an observational note. He also tosses readers a handful of mechanisms that could explain, in a more precise way, why meat might chop down the human lifespan—proposing excess leucine, overmineralization of cells from heme iron, high blood urea nitrogen (BUN), and IGF-1 as the chief contenders.
Those last three—overmineralization of cells, BUN levels, and IGF-1—aren’t worth a particularly deep discussion here. We’ve already covered heme and IGF-1 in the cancer section, and BUN levels are linked not only to animal protein intake, but also to kidney disease, kidney damage, and other conditions that impact renal function (like diabetes and heart failure). In other words, stuff that might independently increase risk of early death. (Although Davis tries to argue that higher BUN levels from eating too much animal protein could somehow lead to earlier death, one of his own references states that “BUN is not a direct factor in the pathway of system dysfunction”—just a marker for existing disease states (179). In other words, animal protein is unlikely to influence death risk by way of BUN levels—unless, perhaps, those BUNs are sandwiching a McDonald’s Big Mac.)
Leucine, however, is worthy of some attention! In discussing the link between calorie restriction and longevity, he notes that it’s probably not eating less food that works some life-extending magic, but the restriction of certain amino acids: “it appears that leucine, an essential amino acid found predominately in animal foods, may be the real culprit in cellular degeneration” (page 234).
We’ve already looked at methionine as a potential life-shortener—at least in rodents, and when eaten in excess or not properly balanced with other amino acids like glycine. But leucine is a far less discussed player in the longevity field. To support the leucine hypothesis, Davis cites several studies suggesting this amino acid can increase target of rapamycin (TOR) signaling, believed to be a key player in the aging process (180, 181)
Rather fascinating, really! There are just two problems.
One, other studies suggest leucine may actually have a pro-longevity effect by enhancing autophagy—the body’s cellular cleaning and recycling process, increasingly believed to influence lifespan and protect against disease (182) (183). And two, some of the highest-leucine items out there are legumes—the very wonderfoods Davis cites as common denominators among the world’s longest-lived populations. If we avoid animal foods on account of their leucine content, beans and lentils would get the boot, too.
So, is leucine worth limiting? The jury’s still out—but the evidence doesn’t seem particularly compelling at this point.
Gone Fishin’? The Role of Seafood in Health and Disease
 As someone who—judging by my restaurant receipts—is single-handedly keeping the sushi industry afloat, I was antsy to see what Davis had to say about fish. After all, creatures of the sea are decidedly high in animal protein! And if there’s something inherently harmful about the collection of amino acids in sentient beings, we’d expect to see a trail of death and destruction in fishes’ wakes.
As someone who—judging by my restaurant receipts—is single-handedly keeping the sushi industry afloat, I was antsy to see what Davis had to say about fish. After all, creatures of the sea are decidedly high in animal protein! And if there’s something inherently harmful about the collection of amino acids in sentient beings, we’d expect to see a trail of death and destruction in fishes’ wakes.
Alas, fish seems to be all but swept under the rug in Proteinaholic. Throughout the book, seafood gets only scant mention—typically with broad, unreferenced statements that do little to negate the many health perks fish has been associated with. For instance, Davis writes:
“Fish were also living creatures, large-scale fishing was an environmental disaster perhaps even worse than livestock farming, and farmed fish meat was just about as harmful to my health as any other kind” (page 48).
“There’s nothing good in fish that we can’t get from plants, minus the sky-high mercury levels that appeared on my blood tests during my pescetarian phase” (page 48).
Additional minor—and rather unconvincing—references are sprinkled throughout the book. Recounting the EPIC-Oxford findings, Davis concedes that “fish consumption also appeared protective” against colorectal cancer, but quickly suggests the finding could be due to fish displacing more harmful items rather than anything inherently health-promoting in seafood (page 207). He claims that due to ocean pollution and modern aquaculture practices, “The result is fish with dangerously high concentrations of heavy metals in their fat”—despite the fact that many fatty fish species are extremely low in mercury (page 274) (184).
In discussing the National Institutes of Health-AARP finding that chicken and fish seemed “protective” against certain cancers when used to replace red meat, Davis encourages readers not to get “misled by people who use this data to promote fish and chicken consumption” (page 213) (185). He proposes a wobbly chain of logic to keep fish on the bad-guy list: because most fish Westerners eat is farmed, and because farmed fish has a less favorable fatty acid profile than wild-caught fish, fish should therefore not be considered a health food. More specifically:
“Wild-caught fish have long-chain fatty acids, which may provide a protective effect because the greater concentration of omega-3 decreases the important omega-6/omega-3 ratio, decreasing inflammation. But most of the fish we get in the United States are farmed. They get omega-6 fatty acids from their grain feed, rather than the omega-3s they would get from their natural diet of algae. These omega-6s are not anti-inflammatory and therefore are not protective against cancer” (page 213).
Putting aside, for a minute, that Davis is accidentally making a great case for eating wild-caught seafood, this paragraph is riddled with unsupported assumptions.
One, although there’s legitimate concern with pollutants and toxin contamination in seafood from certain regions, farmed fish still have a decent omega-3 content. They generally eat a mixed diet of grain, fish meal, and plant foods, so it’s not like they’re mainlining omega-6 fats and ingesting nothing else. In fact, they often have comparable omega-3 levels to their wild-caught cousins, and common species like salmon still contain three to four times as much omega-3 as omega-6 (186, 187). Far from a scaly wasteland bereft of beneficial fats!
Second, studies of farmed fish—provided they’re raised appropriately—show their nutritional profile “is at least as beneficial as that of wild fish” and may even come with some additional advantages (188). The notion that they’re not anti-inflammatory and offer no disease protection is unfounded.
 Third, if Davis is denigrating fish for their omega-6 content, it logically follows that grains, plant-based oils, and even most nuts and seeds (all of which he includes in the recipe section of Proteinaholic) should also get kicked to the curb. For instance, even when farmed, salmon has a higher omega-3/omega-6 ratio than almonds, pecans, pistachios, pumpkin seeds, sesame seeds, walnuts, and similar fare (189).
Third, if Davis is denigrating fish for their omega-6 content, it logically follows that grains, plant-based oils, and even most nuts and seeds (all of which he includes in the recipe section of Proteinaholic) should also get kicked to the curb. For instance, even when farmed, salmon has a higher omega-3/omega-6 ratio than almonds, pecans, pistachios, pumpkin seeds, sesame seeds, walnuts, and similar fare (189).
Davis also makes a rather peculiar statement about wild-caught fish, which—confirming the importance of fact-checking this book—relies on a citation that actually says the opposite of what Davis claims it does. He writes,
“And even wild-caught fish are not an unmitigated health food; even studies that find significant protective effects recommend limiting consumption to two servings per week because of heavy metal, PCB, and dioxin contamination” (page 213).
As evidence, Davis refers to a 2006 review titled “Fish intake, contaminants, and human health: Evaluating the risks and the benefits” (190). Contrary to Davis’s assertion, the paper never recommended capping fish intake at two servings per week: it only emphasized that even this modest level of consumption can confer benefits. In fact, the researchers’ verdict was pretty glowing for all things aquatic:
“Levels of dioxins and polychlorinated biphenyls in fish are low, and potential carcinogenic and other effects are outweighed by potential benefits of fish intake and should have little impact on choices or consumption of seafood.”
“A variety of seafood should be consumed; individuals with very high consumption (≥5 servings/wk) should limit intake of species highest in mercury levels.”
“For major health outcomes among adults, based on both the strength of the evidence and the potential magnitudes of effect, the benefits of fish intake exceed the potential risks. For women of childbearing age, benefits of modest fish intake, excepting a few selected species, also outweigh risks.”
“Avoidance of modest fish consumption due to confusion regarding risks and benefits could result in thousands of excess CHD deaths annually and suboptimal neurodevelopment in children.”
Davis’s statement about “limiting consumption to two servings per week” is probably a misinterpretation of the paper’s advice for pregnant women: “Women of childbearing age and nursing mothers should consume 2 seafood servings/wk, limiting intake of selected species.” Rather than a maximum, though, this appears to be a minimum goal to achieve, since—as the paper explains—the DHA and EPA in fish is so critical for early neurodevelopment in children.
All that said, Davis does offer some potentially noteworthy citations on the fish front! First, he writes,
“A recent review of the literature suggests that a diet high in seafood does not lead to less heart disease and may lead to worse health!” (page 102)
Here, Davis cites a 2014 paper called “’Fishing’ for the origins of the ‘Eskimos and heart disease’ story: facts or wishful thinking?” (191) Although it’s a fascinating read, the article doesn’t actually conclude that seafood worsens health. It merely examines the origin of the “Eskimos rarely get heart disease” narrative and finds the research that birthed it—a series of publications by Bang and Dyerberg in the 1970s—to be flawed. Apparently, the illusion of heart-disease-freeness among this population was a result of inaccurate death certificates and mortality records.
So, the “review of the literature” wasn’t a review of seafood studies, but of papers citing Bang and Dyerberg’s research for things it didn’t truly support. This ties into the important (and oft-ignored) reality that the Inuit aren’t the stunning picture of health they’re sometimes portrayed as, but it also doesn’t imply a high-fish diet per se will tank our health, as Davis alleges. (In fact, the researchers propose that another component of seafood, the amino acid taurine, is highly cardio-protective.)
Next, Davis discusses the Vanuatuan people of the South Pacific, noting that—in one analysis—increased consumption of canned fish was strongly correlated with weight gain (page 111) (192). From this, Davis asserts that “increased animal protein was a key factor in obesity” for residents of this lovely tropical archipelago.

Alas, we’re looking at another case of mistaken conclusion-identity. According to the actual paper, the fish and obesity connection probably had little to do with fish itself:
“Both the nutrient content and the preparation methods of tinned fish likely contribute to its association with obesity. Tinned fish canned in oil or sauce has higher fat content than most types of fresh fish. … tinned fish and meat are often served with instant noodles and rice.”
The study also found that fresh animal products like meat and poultry were associated with lower obesity measures (including waist circumference and sum of skinfold values)—further casting doubt on the idea that animal protein was really the problem here.
That pretty much covers it for Proteinaholic’s potential strikes against seafood. Bottom line? Aquatic creatures still earn a much-lauded place in the human diet!
Summing It Up
Looking at the collective body of Proteinaholic’s citations, Davis’s arguments, and the primary research the book purports to draw from, a few take-home points emerge:
- Avoiding animal protein in order to get healthier has virtually no supportive evidence—but that doesn’t mean an unscrupulous meat free-for-all is a good idea, either. Cooking method, meat quality, and nose-to-tail eating (rather than feasting solely on muscle meat) all make a difference, as does overall dietary context.
- A few health concerns with meat do exist! Excessive heme iron, carcinogens created during cooking, and potentially Neu5Gc could lurk behind observed correlations between certain meat products and chronic disease. Omnivores would be wise to limit their exposure, when possible.
- Fresh, whole plant foods can offset many of those concerns with meat by contributing chlorophyll, micronutrients, phytochemicals, and other compounds to the dietary landscape. Basically, vegetables are awesome.
- Despite some Paleo and low-carb arguments to the contrary, legumes are probably pretty great!
- Rather than a bursting-with-protein killer, seafood appears to be a healthy adjunct to nearly any diet (those who go anaphylaxis notwithstanding—y’all just focus on staying alive, please).
Ultimately, Proteinaholic is a mixed bag—useful mainly for readers willing to think critically, fact-check scrupulously, and spend some extra time separating the wheat from the proverbial chaff (or the cartilage from the soup bone; whatever strikes your fancy). If that sounds like you, grab a copy!
And lastly: a GIANT kudos to Garth Davis for the tremendous amount of work he put into this book, and for adding some fresh material to our ever-churning “I can haz animal protein?” debate. The truth is out there, as the X-Files remind us—and keeping an open mind is the only way to find it.
ADDENDUM: After finishing this critique, I contacted Davis to see if he’d changed his mind about anything post-book publication. He kindly offered the following comments:
- Proteinaholic is intended for the general public (i.e., people who don’t run 20 miles a day or have a second residence at 24 Hour Fitness). Davis acknowledges that the athletic literature is a lot more nuanced and that he’s not well-versed in it.
- Since the book’s publication, Davis became a little more impressed with the value of increasing protein during calorie restriction in order to preserve muscle mass.
- He’s become interested in the low-carb research coming out of Duke University, and thinks there might be something to the idea that there’s “magic” at the extreme ends of the macronutrient spectrum. (He still questions the long-term effects on health outcomes other than weight, though.)
- Direct quote: “All in all I stand by my thesis. I have opened up to the other points of view but still practice what I preached.”
That said, this critique focused only the material as presented in the book, rather than Davis’s potentially updated opinions. And for the record, the few personal exchanges I’ve had with Davis in the past have been entirely thoughtful and cordial: I find him to be one of the most open-minded voices in the plant-based diet community at this point, and am curious to see how his personal stance evolves in the coming years. Thanks, Dr. Davis!

A lengthy post indeed! A quick skim looks great, but I’m a slow reader. Will have to come back and digest a bit. 🙂
Ditto.
These matters greatly interest me and I am very grateful that someone with Denise’s wonderful anylytic and research skills can help me understand these issues to a level I could never achieve by myself. She does it with a mind that does not polemicize but looks at every claim and study on its own merits and never claims certainty where it does not exist. Such enlightenment on my behalf is worth paying for which is what I will do on her website.
A thoroughly comprehensive analysis by Denise as usual….many good points…however, lest we not forget, we are all biologically unique…”one man’s meat is another man’s poison”….there is no one-size-fits-all diet, never has been and never will be…there is a clear lack of understanding about metabolic typing by most ‘diet’ authors….my metabolism tolerates neither legumes nor pulses….soaked & sprouted makes no difference whatsoever…there’s a reason we make up nursery rhymes about them: beans, beans, the magical fruit….
>there’s a reason we make up nursery rhymes about them: beans, beans, the magical fruit….
Why? Do we need to exorcise them, to chant spells before we eat them?
Most folks do not have the necessary enzyme array to digest legumes….that’s why they give people gas…..hence the nursery rhymes…no amount of chanting will overcome digestive inability…
Thank goodness for a new and long-longed for post by Ms. Minger. Denise your posts are a lifeline as I fear that I am stranded in the company of many (otherwise lovely) Militant Marin County Vegans.
Love your posts – and your well-reasoned and civil takedown of yet another T Colin Campbell 🙂
In spite of the friendly words at the end this must be one of the most thorough thrashings a nutrition book ever got – and it appears to be well deserved both on a scientific and a personal level (I mean it serves him right for trying to put you down as some obscure school teacher).
Well, Denise, I am not so sure about the “brief” part, but very interesting. Of course, Davis is by no means the first condemning protein. There have been many others banging this inevitable drum the last several years. All of the macronutrient bashers are, truly, self-serving idiots. They conveniently over-simplify, ignoring the facts that genetics, gender, age, and many other factors, change our needs for fats, proteins and carbs. They also conveniently ignore the facts of human evolution — whether its’s the Colin Campbells trying to make the case humans evolved as vegans (they didn’t), or the body-builder-Paleo dudes pushing books making the case that we evolved eating mammoth steaks (we didn’t) and never touched grains (we did and have been grinding them into flour for at least 35,000 years) or sugars (some primitive folks ate great gobs of honey when it was available), or the vegans that insist that our animal protein intake consisted primarily of bugs (it didn’t), not one of them has an evidence-based, scientific leg to lean on (and I’m sure their desire to sell their books and services never taint their perspective. Right). If we look at the foods on which man actually evolved, the common denominator is that those foods were natural, unprocessed, lightly-cooked for the most part, not fried, etc. And, they included a huge range of fats, carbs and proteins. And most were in the ineptly named “swampland” range. Really. These bozos should check out the meaning of “omnivore”.
Denise, the question on most of our minds is when Part 2 of your “In Defence of Low Fat” series will be published on your blog.
I understand the amount of effort involved in meticulously writing such a paper so please take your time but know that we are eagerly waiting for it! =)
Regardless of his stance on anything, it’s another unfortunate case of someone who is in a way more harm than help to their own stated cause, simply because they can seem totally reasonable until their cause is actually in focus, at which point they become a frothing mash of their existing biases and promptly set up enough errors, strawmen and more obvious targets to kind of make a mockery of themselves and their cause — which I’m sure is regretted by others who share their cause! Thank you for all this work Denise. I recommend two parts in the future.
I recently read the following by Nora Gedgaudas and would like to know your thoughts on this.
http://www.primalbody-primalmind.com/protein-how-much-is-too-much/
Research in just the last few years revealed a metabolic pathway that wasn’t known about before. This discovery revealed a new perspective on dietary protein that, together with insulin–can powerfully influence reproduction, aging, as well as susceptibility to degenerative illness and even cancer.
Cynthia Kenyon’s important work back in the mid-1990’s revealed conclusively that the minimization of insulin is the single most important factor toward the enhancement of longevity and health. No small finding–even though it was hardly headline news (I could be persuaded by a conspiracy theory or two as to why it wasn’t at the time, but I digress). Her work pretty clearly showed the primary reason that caloric restriction–the single most effective of all anti-aging approaches–actually worked. –But it turns out there’s a secondary reason that caloric restriction seemed to confer a marked improvement in health and longevity, and resistance to degenerative processes and cancer.
It has to do with something scientists found called mTOR–which stands for mammalian Target Of Rapamycin. I talk about this in my book at considerable length and won’t overly go into it here. Suffice it to say that this newly discovered metabolic pathway, “mTOR”, apparently serves as a sort of metabolic “protein sensor”. It belongs to something called the “P13K” pathway that is activated by insulin, nutrients and growth factors. It turns out that keeping mTOR down-regulated–by limiting protein intake to what is simply necessary for maintenance–is actually part of the key to maximizing our internal repair and regeneration, immune function–enhancing longevity, anti-aging and minimizing the risk of cancer. Coupled with maintaining low insulin levels, keeping the mTOR pathway largely down-regulated helps keep deterioration and disease at bay and helps keep us young. Ironically, dietary fat has no negative influence here.
That analysis is only about half right. The key in general to keeping disease free, slower aging, or I guess the better word is just general longevity so we live longer is keeping lower levels of circulating T3.
Your thyroid produces T4, and T4 either converts into T3 or reverse T3 (RT3). T3 is basically the metabolic switch that allows one burn off carbs(glycogen), and fats for energy. RT3 basically stimulates the breaking down of muscle tissue for energy.. which is what we don’t want.
Higher circulating levels of T3 are linked to shortened life spans, aging, and disease, but there is an advantage to have periodic high circulating levels: weight loss. You need higher levels of T3 to physically burn off fat (including the stubborn fat). Higher circulating levels of T3 aren’t just based off one pathway (mTOR), it’s based off all the pathways and Cortisol (which is even a bigger influence).
Things that increase T3 are calorie heavy diets, high carb diets (like possibly vegetarian), eating many meals a day, a lot of sleep, or simply a disease that makes the thyroid over-active. This is probably why vegetarian heavy diets have shortened lifespans, they have higher circulating levels of T3.
Things that reduce the amount of circulating T3: calorie restriction, low carb for too long, intermittent fasting, not enough sleep, and over-exercising. The thing is, studies have shown through a diverse cross-section of life that calorie restriction and intermittent fasting increases longevity because it reduces the amount of T3.
Think of it this way, think of a really bright light in your room that has the ability to dim. If you keep your light at full brightness all the time it will burn out quicker. If you dim it or turn it off sometimes, it will last longer. Same thing applies to humans; if our metabolism is ramped up through high T3, we burn out quicker. If it’s slowed down, we live longer. It’s a catch 22, does somebody want to look like a muscular defined statue and live a shortened life, or does someone want to tone it down and live longer?
As I said, it’s not just one pathway, it’s all of them. Our bodies work in a unique way that all these pathways intertwine into our metabolism. Now it is true, we do not need the amount of protein we think we do. Like those people eating 150g-300g daily is pointless, but we do need some or else we suffer from muscle tissue breakdown. Eating too much beyond what your gut and liver can handle will cause a cascade of negative reactions. It all has to be done in balance based on the individual themselves, there is no one size fits all.
As a soon to be endo, I laughed my head off on this comment.
Holy shit, you people (commenting) are cultists! The people convinced that plant foods. fibre and grains being bad for gut health and meat and fat being good for heart health are appalling. It’s like those climate change deniers like someone below said.
WTF: It is certainly true that plant foods are good for gut health; the indigestible (by humans)soluble fiber they contain is digestible by the bacteria in our colon, and in fact is an important food source for them; in return they produce butyrate and other healthful compounds for the human who gives them a home. Additionally, plants are rich in phytonutrients, essential for optimum immune function. I recommend everyone eat a large variety of lots of them. It is also true that meat and animal fat are good for health. Fat provides energy and some vitamins, and meat (including seafood) is the most nutrient-dense of all, containing all the necessary amino acids, and many vitamins and minerals. We evolved eating both meat and plants. There is a reason humans evolved such big brains that, unlike all other species, leads to our being born long before we are ready to live independently. At some point in the dim past our ancestral species discovered how hunt more effectively, how to gather mollusks and catch fish, and to cook all of it to increase the bioavailability of the nutrients, and in the case of large land animals, make it more chewable. The cooking and eating of meat clearly led to the evolution of the human species.
exactly
Joan Mercantini: Very interesting! Tim Noakes had a fascinating recent post, referencing in particular Dr. Reaven at Stanford’s work, that calls insulin resistance the beginning point for, not only diabetes, but heart disease, and more. Take a look at it.
Outstanding, Denise!
Oh dear, what a connundrum. My husband had a 90% coronary blockage and needed four stents, so who should I take dietary and health advice from – a 20 something woman without one qualification in medicine, science or nutrition, or highly experienced doctors and professors, with multiple (and recongnised), educational achievements and many years of experience in their chosen fields? Perhaps they should also let people who’ve just read an awful lot about jet engines service passenger planes too, because hey, let’s not discriminate against people who can’t be bothered (for one reason or another), to get formally trained and experienced. That would be safe enough, wouldn’t it? You could take it further as well. I mean, I guess it would also be OK if your surgeon had just read a few books (and had an interest in the subject), because it would be terribly elitist to demand he/she actually had a medical degree? I honestly think people with the arrogance to try and charge people for health consulting (as you do on your site), without having any formal qualifications, must have mental health issues. Narcissm is the first issue that springs to mind.
I hope your husband gets the medical care he needs to get better. All the best.
90% coronary blockage + four stents… and you are still listening to the advice of “highly experienced doctors and professors”? I believe it was Albert Einstein who once said “Insanity: doing the same thing over and over again and expecting different results”. Perhaps you should consider changing your strategy – perhaps listen to this 20 something woman here?… – do not be fooled by age (or formal degree) Kim! Stupidity is the first issue that springs to mind!
Aviel, believe me, he didn’t get the 90% coronary blockage and need 4 stents because we were following any expert medical and nutritional advice, quite the opposite. You think coronary artery disease is the number one killer in industrialised nations because are listening to qualified advice? That’s ridiculous for you to assume. It was only after the proverbial hit the fan that we turned on a sixpence and paid attention to the likes of Dr. Kim Williams, Dr. Caldwell Esselstyn, Prof T Colin Campbell and Dr. Garth Davis. Since then, he’s lost 16 kilos, dropped 3 waist sizes, seen his overall cholesterol drop below 3mmol/L without statins (that’s our Australian scale) and stayed free of the painful angina he had before. So tell me Aviel, would you be content to let an unqualified pilot fly your next holiday jet across the country, or an unqualified surgeon open up your abdomen in a medical emergency because you’re not fooled by age or formal degrees? Maybe you could suggest that to airlines and hospitals as a way of saving money?
moriganne: Losing weight, and especially waist size, is a very good thing, but cholesterol that low is very dangerous, I repeat, very dangerous. Take a look at the American Heart Journal, Volume 157, Issue 1, Pages 111-117, January, 2009, “Lipid levels in patients hospitalized with coronary artery disease: An analysis of 136,905 hospitalizations in Get With the Guidelines”
These were patients admitted with heart attack or unstable angina. Look at the data: The highest risk was for those with LDL between 2 and 2.75mmol/L, at all levels of HDL. The lowest risk was for those with LDL greater than 4.4 at all levels of HDL. Past age 50, high cholesterol is protective, especially in women, but in men as well. Then read Denise’s posts about T. Colin Campbell. I personally wouldn’t believe a word he said. Then read the blog posts of Dr. Malcolm Kendrick (a Scottish doctor). Cholesterol level, except for those homozygous for familial hypercholesterolemia, is an entirely useless predictor of heart attack risk, since cholesterol is not causally linked to the development of heart disease and it plays many vital and critical roles in our health. A much better indicator is the level of insulin resistance.
@Gary – cholesterol tends to be usefull in fighting infections.
http://suppversity.blogspot.com/2016/05/cholesterol-boosts-your-immune-defenses.html
GTR: Absolutely. This is likely one of the major reasons high cholesterol is associated with longevity. Also, cholesterol sulfate is the precursor for vitamin D sulfate synthesis in the skin, and for sex hormones. Cholesterol is such a crucial molecule for metabolic health and the structural integrity of cells that our fifty year obsession with lowering it is absolutely nuts! For men over 55 and for women of all ages, high cholesterol is protective. This is a well-established fact. But medicine in our world is run by pharma, not by facts, or by what is best for the patient. I owe my excellent health to doing the opposite of what the government says (about all things scientific, medical, and nutritional). Prescribing statin drugs to men over sixty and women of any age is practicing quackery.
And don’t forget that people with low cholesterol, 160 or below, die from more causes overall, including suicide (cholesterol is necessary for good brain functioning), than people with high cholesterol. And it has been shown that murdering psychopaths tend to have low cholesterol.
Hi Gary, I’m at bit confused by your statement “The lowest risk was for those with LDL greater than 4.4 at all levels of HDL.”. The conclusions from the study itself state rather simply: “These findings may provide further support for recent guideline revisions with *even lower LDL goals* and for developing effective treatments to raise HDL.”
This video should very clearly demonstrate why you don’t want to raise your LDL.
http://nutritionfacts.org/video/optimal-cholesterol-level/
I think the issue with your reasoning is that you’re saying a small percentage of the people admitted to hospital with CAD events had extremely high LDL and therefore we’ll be better off if we have extremely high LDL. But you fail to realize a very basic point, which is that if there are only 1,000 people in the world with LDL>4.4, and they ALL have CAD events, it’s not a healthy way to be! You need to answer the question “What percentage of those with LDL>4.4 have CAD events?”, not “What percentage of those who had CAD events had LDL>4.4?” Let me know if you have any questions, it’s best not to spread dangerous misinformation like this, people’s lives are at risk.
Jeff Robertson: In the AHJ paper I referenced almost 50% of the 100,000+ patients had LDL within the guidelines (<100mg/dL). Serum cholesterol levels have no reliability as predictors of cardiovascular disease or events; blaming cholesterol (as the authors do in the first sentence) for causing atherosclerosis is like blaming the firefighters for the fire. TC/HDL and TG/HDL ratios do have predictive value, but only because they are surrogates for the metabolic dysfunction which leads to CVD. I am not advocating anybody raising their LDL, nor have I any idea how one would do that. There is abundant evidence, however, that for those over 60, high cholesterol increases longevity, and low cholesterol reduces it. Like many other clinical interventions, the purpose of cholesterol testing and reduction is profit, and nothing else. It is the medical industry and their lapdogs in the media and regulatory agencies who are spreading misinformation, not I. They are destroying the nation's health from the womb up.
Gary Ogden: We know that reducing the amount of SF and cholesterol in one’s diet reliably reduces LDL, and that this reliably reduces the progression of atherosclerosis … we have 395 metabolic ward studies proving the first point:
https://www.ncbi.nlm.nih.gov/pubmed/9006469
and we know from multiple direct measurement studies that atherosclerosis does not progress when LDL is under 75 mg/dL on average, and progresses in a linear fashion for any increase in LDL above 75. Here are data from 7 separate studies showing this clear linear relationship:
http://www.onlinejacc.org/content/43/11/2142
Click to access 2757.full.pdf
so, all told, i see good reason to lower one’s LDL cholesterol, since it stops the progression of heart disease. what better reason could one need?
therefore, i see insufficient evidence to say that ‘the purpose of cholesterol testing and reduction is profit, and nothing else’. Let’s be honest, this is not a serious statement, but rather a conspiracy theory. If you have evidence in support of this alleged world-wide conspiracy of all doctors across all nations and languages to collude to lower everyone’s cholesterol for no reason other than profit, I’m all ears.
Some minor corrections, Jeff. Does not progress under 75… on average. It can. A second point is the first paper noted a concomitant drop in inflammation. This cannot be assumed to be due to a drop in LDL as statins have this effect anyway and many now believe that this is their main mode of action, the LDL lowering being a surrogate for it.
Thirdly, despite all of this, LDL does not correlate with CAC scores nor with radiographical assessments of atheroma, nor with post-mortem atherosclerosis burden. If LDL was the MAJOR driver of atheroma, I imagine it should be.
What lines up in all the data is insulin-resistance. This is the gun, and some of the bullets are LDL. Treating the LDL as the primary therapeutic target has indeed some benefit, but tackling the IR has more.
A recent trial comparing three weight-lowering diets including low carb showed equal atheroma reversal in carotids. This wasn’t intimal thickening but actual atheroma. It was postulated that the main mechanism was blood pressure lowering due to weight loss.\
If LDL lowering is so important, answer these.
Why in Predimed etc., does this “Mediterranean” diet do better than statins with NO cholesterol lowering?
Why is heart disease in the Gascony area of France so low despite average cholesterols and huge consumption of satfat?
Why is the heart disease in Japan falling even more as they eat more satfat?
The clue to some of these of course is probably that HDL is raised by satfat, and if you’re eating a lot of fat, you’re eating less sugar/carbs.
The Framingham model shows only a weak correlation between CVD and total cholesterol. The model shows strong benefits for reducing CVD from raising HDL and lowering systolic blood pressure. Chasing LDL is not as helpful as working on the other two. But it’s easier for most people to take a statin than walk 10,000 steps a day.
Education is not limited to those with degrees. To think that those ‘most educated’ are those with the ‘most degrees’ is to not be educated yourself!
It’s also interesting that none of the doctors you mentioned are YOUR doctor, but research doctors who (wait for it) mostly do studies and education, and then practice based on what they learn in their studies, but that is contrary to what is taught in their education. In fact, doctors get about 2 hours of education on nutrition in their career. So to be taking educational advice from doctors who study nutrition is decidedly taking advice from someone who was not trained in nutrition and are just like ‘pilots without training’.
Nutrition is not a ‘skill based’ occupation, like flying, but an EDUCATION based occupation. I might very well trust a self-taught mathematician to teach me math, while still preferring my pilots to be well-trained in flying and to have taken flying courses. That’s because math is education-based, not skill-based. They are not equivalents.
Degrees do not confer education. Education does. A degree is only a body stating that one has a minimum level of a particular education. But not having a degree does not mean that one has not achieved the same or higher level of education. In fact, many of the best thinkers in the world did not receive degrees or education in their chosen fields.
Edison, for instance, was kicked out of elementary school for being virtually retarded, and his education was almost completely of the self-taught variety. Yet every day you recklessly turn on light switches that were invented by a non-electrical engineer!
Plus, everything you said is a logical fallacy. You did not state that Denise is WRONG in any of her statements, you merely implied that she MUST be wrong… because she doesn’t have a medical degree! Despite the fact that those with the medical degrees you are citing did not get their nutrition training in medical school!
You ALSO did not even give an N=1 anecdote and say, “We tried her advice and my husband’s cardiac risk markers went for the worse”, you just said that they improved by taking the advice of those you mentioned. However, no where does Denise claim that a vegetarian diet would make cardiac risk markers worse, in fact, I’m sure she’d agree and argue that they’d improve on a plant based diet over an SAD diet.
Her argument is not that vegetarian diets will kill you, only that adding responsible meat consumption will NOT increase the risk, and may even improve the risk over a vegetarian diet. However, ALL Of these sources agree that eliminating junk foods and processed foods will improve cardiovascular markers- which is almost certainly what your husband did.
So, your entire argument is a fallacy as well as being contradictory. You’re claiming that only medical school can give one the education and right to teach nutrition, however, you’re taking advice from doctors who decidedly did not learn their nutrition in medical school, but on their own.
Love your comment Kerri, I have put into a file for reference.
Hi Kim, my late husband who was T1 diabetic had a quad bypass and after his operation the hospital fed him the standard high carb diet. I wrote to Dr PeTer Attia for advice, and he recommended. Low carb, moderate protein high fat diet. Hope this helps
Perhaps that’s why he’s your late husband?
Oh my God you are just a mean troll.
how absolutely vicious and unnecessary.
Kim Bax: With this book, Garth Davis is stepping completely outside his area of training, expertise, or competence. Physicians are given almost no instruction in nutrition or the biochemistry of food in medical school. My own family physician is first-rate, and I trust her completely, but I am the one who has trained her in nutrition. And I’ve got news for you, neither stents nor CARBG’s extend the lifespan. Only lifestyle changes, primarily nutritional in nature, do that. Your letter is seething with the arrogance of the ignorant. I trust what Denise Minger writes because she provides all the relevant evidence (how many doctors do that?). This is science. Science is based upon evidence; the more the evidence, the stronger can be our confidence. Yet for all of my lifetime since my teen years we’ve had the diet-heart hypothesis shoved down our throat, but there was never any confirmatory evidence, and evidence that would have falsified it thoroughly (Minnesota Coronary Trial) was buried, unpublished, by Ancel Keys himself; he bullied anyone who disagreed with him, attained a position of authority with the AHS, and this nonsense was etched in stone, until Ramsden and Zamora recently unburied it, reanalyzed it, and discovered that for every 30 point drop in TC, the risk of death rose 22%. This is why he buried it, because it demolished his hypothesis. I most certainly wouldn’t trust a cardiologist, unless my own research showed that he or she knew what the hell they were doing.
In your opinion Dr. Garth Davis is stepping outside his area of formal expertise so you put your faith in someone who has absolutely no formal expertise? And you say doctors have little training in nutrition, so you put your faith in someone who has zero? That makes sense (not). Prof T Colin Campbell is one of the most highly qualified nutritional experts in the World and Denise tries to rubbish him as well. As for the “News” that heart surgery doesn’t prolong life, I’m aware of that, but when people are diagnosed with massive coronary blockages after major heart attacks or crippling angina (which in most cases strikes completely out of the blue), they’re often too panicked and frightened to refuse surgical intervention. The research and thought comes afterwards. Further, every recognised nutritional and medical authority in the World agrees that diets high in animal products (and fatty processed foods), plus low in whole plant foods, leads to heart disease. The science is in and the argument is over. This continued “Debate” is eerily similar to the Global warming “Debate” (where again, the science is in and the argument is over). You read similar stuff from poorly qualified (or unqualified), denialists/outliers (and cranks) in every corner of the internet saying everything’s fine and the climate’s right on course. They quote and reference to sound authoritative (like you above on diet and heart health), but someone with real qualifications and background can unpick it in an instant. Further, as with the Global warming “Debate,” the rare poorly qualified oddballs who think diets high in animal products (and fatty processed foods), have nothing to do with heart disease are given hugely disproportionate publicity, given their tiny minority opinion and lack of credentials.
PS Quote: “Your letter is seething with the arrogance of the ignorant” – the only thing that’s arrogant and ignorant is someone with zero qualifications in health asking people for money, so she can advise on vital issues which she’s not trained in. Is it also “Arrogant” and “Ignorant” to expect your pilot, aero engineer and/or surgeon to have formal qualifications and education? I think not.
moriganne: Denise Minger is a very bright young lady. Have you never heard of self-education? Some of the greatest scientists in history (including the greatest, Isaac Newton) have been self-educated. I suggest you read all of her posts, read all the scientific papers she references (and clearly understands) before you have the temerity, the gall, the effrontery to belittle her again.
moriganne: Science is never “in.” To say something like that is to show a misunderstanding of what science is about. But there is no sense debating with a true believer. What T Colin Campbell and the rest represent is religion masquerading as science. Widely recognized authority? Only in the Church of Veganism.
Moriganne,
the French, Swiss, Spanish paradoxes. The Gascony area of France has half the incidence of CHD of the rest of France and consumes the most satfat in the “civilised” world. All sorts of fabrications are produced to rubbish this fact, but they don’t stand up. Spain similarly eats a good amount and Switzerland.
That there and then shoots you down.
And, by the way, the Kitavans ate 18% satfat and nearly all of it from coconuts and had no apparent heart disease.
There’s a clue in all of this. It’s that satfat is NOT the primary driver of heart disease. The trials showed this, notably the WHI and the buried Minnesota trial.
Satfat does raise LDL in some people but it raises HDL too. It also has a very beneficial effect on LDL particle size.
IMO sat fat is not the answer to CVD problems either.
I lived in south France for two years, eating faty/carby/sugary foods ad libitum. I lost 15-20 pounds during that period. The difference between France and the USA is that I walked everywhere, every day. At least 5 miles a day. IMO the primary factor in “diabesity” is sedentarism rather than diet.
I am sure that you know, that sometimes even two old male doctors or professors have different opinions…
Your contribution to the discussion is nothing (mine also).
Kim, what brings you here then, if you’re so satisfied with your medical “professionals”? It was a couple of high school graduating, bicycle mechanics who developed controlled flight, not degreed scientists or engineers. While we’re at it, where did Hippocrates get his degree? Don’t be so enamored with the sheepskin, that you can’t see the wolf hiding underneath
“My husband had a 90% coronary blockage and needed four stents” – what is your proof for such specific requirement?
Kim- Unfortunately most physicians, by no fault of their own, learn pitifully little, if anything, about nutrition in medical school. Most doctors don’t have much advice to give on the subject. Hopefully this is changing, but the pace of change is glacial. While I wish you and your husband the best, I don’t believe that a personal attack on the author is warranted. We are in an information age now, where biomedical research is published online and accessible to the public. Academic institutions often curate the information on their websites, or we can look up the research ourselves on PubMed.gov. Educated and intelligent individuals such as Ms. Minger can actually read and study the data for themselves to make better decisions about their own health. This is revolutionary, much like the invention of the printing press. It places more power into the hands of the individual instead of blindly trusting in a patriarchal system that thrives off of our helplessness and would like to be seen as a keeper of secret knowledge. If I have certain health issues, I would seek out someone who has personally overcome those same health issues herself. If someone wants to seek out Ms. Minger, that’s his/her choice and they may get much better advice from her than from a fellow in a white coat who has had no personal experience with the issues, and no knowledge of nutrition from his training.
Have you read Denise’s previous post about diets and heart disease? It has a good indepth look at diets and heart disease, including the very-low-fat diets and why they may be “magic” sometimes.
Really though, we all should be doing our homework and hoping people are analyzing this question besides the surgeons. The surgeons and heart doctors at this point don’t have a very good track record … the ones tending to people in my extended family are mainly into pills and scalpels. After a heart issue of my own I asked two different cardiologists: “What should I do different?” and basically their answer was “That’s not our department”.
The people who have been through med school … and there are some in my family … are taught a curriculum that is largely informed by the drug companies. They have for the most part given up on “diet” as a way to treat patients. With a few exceptions … like Esselstyn et al … and I totally give them kudos for bucking the trend with their own peers and experimenting.
Yet, they are still experimenting, and “the” answer is still evolving. The dialog here is part of everyone experimenting. Smart people can research just as well … and maybe more open-mindedly … than a person with a medical degree. And since it is YOUR husband’s heart, it’s up to you to research. If it was me, I would not limit my search to only the people who graduated from med school.
My Dad, BTW, followed the standard advice, avoided saturated fats and sugars, lowered his cholesterol, became vegetarian, ate loads of vegies and legumes, didn’t smoke, exercised daily. Became thin and trim. And his arteries were in horrible shape, his bones were weak, and he got multiple health issues. I’m sure there is “something” wrong with the Standard American Diet, but I’m pretty sure it’s not the currently suspected culprits.
There is an excellent presentation on the fat emperor blog about calcium score (CAC), which, unlike cholesterol or any of the other mainstream “risk factors,” has real predictive value. I’d suggest anyone concerned about heart disease should watch it.
Kim, are you aware of what a logical fallacy is? It’s a failure in reasoning that renders an argument invalid and non-substantial. You used no less than three in one post and without making a valid argument or point of your own.
You start with an anecdotal fallacy, basically implying that because your husband has had success with his treatment, and his treatment runs parallel to the thesis of the book, then any claim against the book and its thesis are invalid.
You then proceed with my favorite: ad hominem. Her being a woman, being in her twenties, or not receiving a degree in a medical field does not, in any way, counter any of her points or claims. Those facts are completely immaterial to anything she wrote. That’s the equivalent of not being allowed to critique the flavor profile of a cake, because you are not a professional baker.
You then proceed with my second favorite: argument from authority. Basically the premise of your argument is that because they are qualified, medical professionals, any claims and arguments they make must automatically be correct or valid. The fact that many of these people are “qualified” yet make completely invalid arguments should probably concern you. It would also stand to reason, given that information, that someone being “qualified” isn’t going to be completely correct or reasonable all of the time on that basis (being “qualified”) alone.
You finish with several comparisons that are, I’ll admit, amusing to read; although, only because they are entirely ridiculous. You compared something that you learn in school (in the U.S. anyways) with something you have to go into specialized training for. It’s very easy to learn how to accurately interpret studies and quote relevant statistics (you can do it too!). Like I said, in the United States’ regular education, you learn all about interpreting studies, reading abstracts, looking at data, determining the importance of p values, etc.. Denise didn’t come up with this data herself, she quoted those qualified, medical people you put so much faith into. Anyone can do that. The rest is just reasoning which, as you yourself have demonstrated, may indeed be limited to only select people.
There are so many of the same old tired, disingenuous, fallacious arguments in this post from “Kim Bax”‘ that I, for one, suspect that the “90% coronary blockage husband” is merely a figment of a very angry “Kim Bax”‘s imagination, in an attempt to make her personal attack on Denise kinda acceptable to unsuspicious readers. Trolling takes many forms.
Thank you for this, as always, charming and edifying, post. My lifetime, but particularly last eleven-year, journey in eating has brought me to daily, smallish amounts of a wide variety of seafood, with occasional gorging; gobs of vegetables, especially wild greens and herbs from the garden, nutrient-dense fruits, pastured animal foods, including organ meats and bone broth. No grains, and legumes only rarely (natto, as revolting as it is, for the K2, and sometimes miso). Works for me! Haven’t been sick in eleven years, and have no diseases. Your blog has been a crucial part of my gaining of dietary knowledge and understanding, along with WAPF (I’m a former member), Mark Sisson, Dr. Mercola, and especially mom, who fed us liver & onions (this was always one of my favorites) decades ago. I say “show me the evidence!” And you deliver. Your blog is a treasure.
Garth is one of those vegans who is willing to bend the truth for his ideals. I don’t admire that. (He’s not the only one). When I acquainted him with Malhotra’s Indian Railway Workers’ study he blocked me on Twitter.
If meat and protein are so bad, how come the population of Hong Kong who eat more meat and also more beef than any country (taking Hong Kong as a country) live longer than any other country, men and women?
Also the French in Gascony eat more sat-fat than anywhere else and get very little heart disease.
He just doesn’t want to know the truth. If you are a scientist you must acknowledge the truth, not create it.
In this regard he falls seriously behind Chris Gardner of Stanford who, though a vegetarian, acknowledged the Atkins diet as being the winner in the A to Z business. Well done, Chris, no marks Garth.
Garth Davis is not a scientist. Science is a way of evaluating evidence, and he either doesn’t know how to , or is not interested in it, or both. Denise Minger is undoubtedly a scientist, even though she doesn’t have alphabet soup after her name.
Nice post – worth the wait!
In the paleo circles I’m familiar with, the issue with legumes does not have to do with weight loss so much as with protein quality and inflammation. Indeed, us long term paleo practitioners tend to forget that the diet tends initially to be used as a weight loss diet, as it has so many other health benefits that can be more important for us older folks who are past the onset of metabolic syndrome.
“Chimps have a surprisingly intricate hunting ecology—patrolling the forest in slaughter-ready groups, scouting out meat even when other food is abundant.”
I’m glad you pointed this out. The “reluctant hunter” narrative that tells us primates tend to seek out meat only when they are desperate for food doesn’t hold up. Plant foods are nearly always more abundant and easier to access, and it could very well be the most well-fed primates who are most likely to hunt.
Chimp culture is complex, and there are “political” ramifications involved with hunting, too. The underpinnings of their meat-eating and hunting behavior is still very much a mystery. This is a pretty cool article about chimps and hunting for those who are interested: http://www.americanscientist.org/issues/pub/chimpanzee-hunting-behavior-and-human-evolution/2
Here’s an excerpt that points to social and nutritional aspects crossing boundaries: “…male chimpanzees use meat as a tool to gain access to sexually receptive females. But females appear to be getting reproductive benefits as well: William McGrew of Miami University in Ohio showed that female chimpanzees at Gombe that receive generous shares of meat produce more offspring that survive.”
On another note, Katherine Milton (whose chimp data is used in your article) wrote a reply to Cordain’s seminal Paleo paper, which was also published in the same journal, The American Journal of Clinical Nutrition. She questioned the ethnographic data as well: http://ajcn.nutrition.org/content/72/6/1590.full
<80% (135) of the 165 “hunting” societies listed in the Atlas.
In contrast, in their analysis, Cordain et al (1) identified 229 hunter-gatherer societies in the Atlas; they also combined 2 of Lee’s discrete categories (hunting and fishing) to estimate the total contribution of animal foods to energy subsistence. Given the uneven quality of most dietary data in the Atlas, the overrepresentation of hunter-gatherer societies from more temperate locales and the differences in classification and data analysis between these authors, different conclusions seem inevitable and all conclusions appear to merit closer study.
The !Kung and Hadza, dismissed by Cordain et al as “unrepresentative,” differ from many hunter-gatherers listed in the Atlas precisely because they have been relatively well studied dietarily—in both cases, plant foods contributed the bulk of daily energy intake.” >>
Chimps look like a wrong evolutionary bath, based on staying in the trees, at the time when the world was becoming a savannah… Primates had a lot of evolution during a very hot, foresty Eocene eopch. Finding plant based food was easy then:
https://en.wikipedia.org/wiki/Eocene
“At the beginning of the Eocene, the high temperatures and warm oceans created a moist, balmy environment, with forests spreading throughout the Earth from pole to pole. Apart from the driest deserts, Earth must have been entirely covered in forests. Polar forests were quite extensive. Fossils and even preserved remains of trees such as swamp cypress and dawn redwood from the Eocene have been found on Ellesmere Island in the Arctic. […]
Cooling began mid-period, and by the end of the Eocene continental interiors had begun to dry out, with forests thinning out considerably in some areas. The newly evolved grasses were still confined to river banks and lake shores, and had not yet expanded into plains and savannas.”
Apes ruled during cooler, but still very hot time of Miocene.
http://www.primates.com/history/
At the end of the period it was clear the forests are out, and dry grasslands are the future. Human ancestors made the right decision where to go. Chimp ancestors made a wrong decision where to stay. So chimps are not necessairly a good example of doing things rigtht…
Oh Denise Minger, how I love you, let me count the ways… 😉
It’s very comforting to know that a young and intelligent woman can rely on her independent research instead of the accredited (uninformed) health authorities. I also love that you aren’t tempted to be condescending when demolishing another person’s life’s work so easily… ;D
Now where’s the second part of your low-fat/ high-fat post? Let it be just as long…
I am eating high fat low carb..I lost 60 lbs with ease….I LOVE my bacon and my cheese and my butter..all of the forbidden foods that I craved but avoided when my weight went up and up and up….I was in a 12/14 now I am a 6/8. I had so many medical issues it was not funny…9 pills a day….now I need ONE….I think this article is a load of crap…I have kept the weight off for over 6 years eating literally as much as I want…every day….I can even cheat some and stay tiny….go watch the movie “Fat Head” it will change your life.
I would love to see your blood work-up. Being thin doesn’t mean your are healthy.
What do you want to see? I’ve also lost 50+ pounds eating as much fat (particularly animal fat) as I can every day, and also using intermittent fasting after about a year of low carb. I’ve been on low carb about three years now. My HbA1c has decreased, as has my fasting blood sugar and insulin, my LDL is around the same (119, 129, 103; these are calculated; had actual LDL taken once and was 91), my HDL has increased 40% (37 to 49 to 52), my triglycerides have decreased (113 to 120 to 65), my TC is around the same (175, 202, 168), my cardiac CRP is 1.29 mg/L (only took it once), my LDL-p is 1184 (only took once). This is after about three years on low carb and these are tests that span that range. I have to pay for anything that’s not a “normal” test, so I don’t get them done that often. For instance, I have to pay for HbA1c, cardiac CRP, LDL-p, etc.
I don’t get the “3pm sleepies”, I’m never tired (except when physically so), I’ve had only minor colds/stomach bugs, etc. I avoid eating all grains (whole or otherwise), I avoid eating seed oils, I avoid eating fruit (makes my blood sugar go through the roof). I eat vegetables and meat and fat. I eat some resistant starch (lowest carb variety possible) and fermented vegetables (these two only in the last year, just to test them — it’s still unclear there’s a benefit or detriment). I will use olive oil and avocado oil and that’s about it. I use duck fat, goose fat, bacon fat, butter to add to vegetables and meats. I eat dairy, full fat yoghurt (make myself if I can), the fattiest cheeses I can find, and cream. Will periodically eat potatoes (heated then cooled then reheated), but not many of these. Will go off this diet every once in a while such as vacations and holidays, but get back on immediately. Try to eat the diet when out and also on vacation, but it can be difficult to do so, as everything is bread and carb related in the US.
“Animal protein, according to Davis, is not the key to weight loss—but rather, a chief cause of our expanding waistlines. Far from making us healthier, it drives the progression of cancer, heart disease, diabetes, and other ailments crippling the Western world”
This is funny because this very thing was discovered over a century ago when tariffs were removed on sugar and it was noted those very diseases described above skyrocketed in the population. Not meat, sugar was the issue.
So my question is, why do people like this repeatedly ignore these studies/observations that have already taken place over a century ago?
Animal proteins aren’t the problem, some Inuit populations prove this by exclusively eating red meat and have no diseases and are lean. Saturated fats aren’t the problem, as evidence by the Tokelau study (only real world study on saturdated fat) who eat 70% of it and have no diseases and are lean. Even a veggie heavy diet isn’t the problem provided someone has a thriving metabolism and gut flora (which doesn’t apply to most people). The problem also is with vegetarian style diets is they do in fact have shortened lifespans by about 10-15 years. Most people never on that eating style due to insufficient nutrients because YOUR GUT CANNOT BREAKDOWN THE FOOD PROPERLY, and this especially applies to grains. This isn’t even debatable because these researchers know full well just how difficult it is for someone to break down even cooked veggies in the gut, let alone grains which is next to impossible. Most people have compromised systems, and the way that is fixed is by eating stuff that is easily digested, and that is cooked meat. It is the easiest on digestion, and you still get the full benefits of the plants or grains that the animal has consumed themselves. Yes the animals have better digestion that we do and can break all that stuff down easily, we can’t, that’s why we eat the animals.
“The problem also is with vegetarian style diets is they do in fact have shortened lifespans by about 10-15 years.”
Okinawans. Mostly sweet potatoes.
Our gut can’t break some things down but our bacteria can.
Are you including white rice as a “grain?”
Who actually eats “grains” though? The whole anti-grains thing is really weird because I don’t know people who eat grains besides rice. When the whole Paleo thing exploded a few years ago, I thought is was weird that they focused so much on something that nobody eats. If by grains they mean flour products, then yes, those are highly refined, cause blood sugar problems and are cooked in fat inherently and always consumed with many others foods at the same time (deli meats, cheese, mayonaise, etc.) But If they mean things like:
Amaranth
Barley
Buckwheat
Farro / Emmer
Kamut
Millet
Muesli
Quinoa
Rye
Sorghum
Spelt
Teff
Triticale
then I don’t know what all the fuss is about because no one eats those things. So one of their central thesis’ is that modern disease is caused by something people don’t even eat? Ok.
WP,I beg to differ with you. There are in fact many of us who eat a whole food plant based diet who eat many of the grain you listed. I just had kamut salad for lunch today and loved it.
Hey WP,
Where do you live ? A LOT of people eat these (pseudo)-grains but maybe not in the US / Canada / UK. I eat buckwheat groats fairly regularly, same with spelt, millet, quinoa and barley. Rice is good but really, I like some variety as well 🙂 but besides me, those are staple foods in many places (Africa, Eastern Europe, Asia, etc).
Okinawans may eat ‘mostly’ sweet potatoes, but they are not vegetarians, getting between 10-15% of their diet in the form of meats, mainly from seafood and pork. They also cook in lard and use animal broths in their many soups. So equating the Okinawan diet as a vegetarian diet is simply factually incorrect.
Also, to say that ‘no one eats grains’ while admitting that wheat is a grain, but ignoring it’s ubiquitousness in the western diet is also dishonest.
This brochure from the USDA states that, from their research, Americans eat over 6 ounces of grains a day. That westerners mostly consume a single grain does not mean they are not consuming grains.
Also, you said, “cause blood sugar problems and are cooked in fat inherently and always consumed with many others foods at the same time ”
Not in the US. A ‘typical’ breakfast might be simply toast with jam, a muffin, or cereal with milk. A typical dinner might be pasta… sometimes served with bread. Westerners eat grains with almost every meal. That is why there is the focus on grains in the paleo diet. Try merely SUGGESTING that a family member eliminate grains and you will watch them struggle with what they might possibly even eat, because they are eating grains in such high quantities as staples that they must readjust their entire thinking to be able to eat without grains.
But the point WP was making, was that (most) people nowadays don’t eat whole grains.The highly refined white flour based ‘grains’ such as breads and pastries, highly refined cereals, muffins etc that are eaten by many people these days are perhaps are not that good for us.
Instead of eliminating grains, why not suggest the family member replace the refined grains with whole grains (eg as in WPs list), and legumes and root veges such as kumera (sweet potato). And eat more fish, and eliminate most added sugars.
One of the problems of Blue Zones model is that these are typically island populations (Sardinia, Okinawa, Ikaria), separated from the mainstream populations; basically with somehow different genetics that the continental mainstream. Even the religious sect example of the blue zones (adventists) becomes “islandised”, as people of the same faith tend to marry each other in next generations after conversion.
Besides plant-based food itself creates selection for different genetics. Notice Europeans are the least vegan of large populations (that is not including small groups like Inuits) based on the proportion of the gene: just 17%, as opposed to 53 percent for Africans, 70 percent for South Asians, 29 percent of East Asians.
https://www.washingtonpost.com/news/to-your-health/wp/2016/03/30/cornell-study-finds-some-people-may-be-genetically-programmed-to-be-vegetarians/
http://www.news.cornell.edu/stories/2016/03/eating-green-could-be-your-genes
Excellent point by WP. The only people I know who eat the above grains are vegans/vegetarians. Most people eating SAD consume white rice, pasta, bread. Denise love your blog, looking forward to Part 2 of the LF article 🙂
fascinating. thanks for your reply.
i had a low carb diet for years, and developed issues with slowed metabolism: cold all the time, hair loss, dry skin, low energy, really slow “digestion” no matter how much fiber i ate. and sitll borderline hba1c. then, after a blood test showing i had really low insulin and leptin levels, i switched to very low fat, higher carb than before (but moderate, really), less protein. vegan-ish without being vegan, still eating occasional meat, fish, and eggs. i feel better–warmer, and immediately started gradually losing weight, especially around the middle.
so perhaps for me, i tend toward lower T3, and need carbs to function well. I would have never guessed, i was so into keto and believed it was the best! i still read about it and want to go back to it, and have to keep reminding myself of the results.
About vegans often showing worst outcomes in various studies. Going vegan requires more education, input, experimenting with foods, than does continuing to eat the same old, an omnivore diet, if maybe cleaning it up a bit. I wonder if many of the vegans–a significant amount–in some under the surface self-selecting way–were sick or getting sick and became vegan because they were already or in process of becoming sick. They, then, would manifest disease, and death, more than others who had no reason to change their status quo.
“They, then, would manifest disease, and death, more than others who had no reason to change their status quo.”
that’s why some of the studies try to wash these possibilities out, and study people like the Adventists who eat vegetarian for religious rather than health reasons, or to compare the health of ‘cultural’ vegetarians vs omnivores; and to study groups of omnivores and vegetarians frequenting health food markets since, ostensibly, omnivores eating healthy would likely choose to eat healthy for the same reasons as their vegetarian counterparts.
These are some of the ‘confounding factors’ that scientists try to account for.
Have you seen Tim Steele’s new book, The Potato Hack? It seems to have universal appeal to vegans and paleo alike. He uses a very short-term vegan approach to fixing damage and losing weight. Judging from his Facebook and Amazon reviews, this book is doing very well. It’s amazing to me that the paleo elite, Sisson, Kresser, and Asprey among others have fully endorsed a 100% vegetarian intervention. That alone speaks volumes. However, as a short-term intervention, it allows for whatever meat one wants normally. Could the potato be the answer to everyone’s problems?
Potatoes are generally considered to be healthful food, particularly in potato salad, since cooking followed by cooling develops resistant starch, which is indigestible in the small intestine, but makes the gut flora in the colon very happy, because it feeds them. For good health it is essential to keep the little buggers happy. Just don’t make the potato salad with commercial mayonnaise, since nearly all of it is made with soybean oil.
I have! It’s awesome, lol. Thanks.
Fantastic read as usual.
Again, Ms. Minger, an excellent critique. I only have two pet peeves and neither one of them have to do with you article, at least, not directly. First pet peeve. I loath the vegan vs. vegetarian designation. Eggs, cheese, milk and fish are not vegetable matter. A vegetarian, by pure definition, should be person who only eats vegetable matter. If a person eats animal matter
they they are not pure vegetarians. They are un-pure vegetarians. 😀 Or, perhaps 80% vegetarians? Second pet peeve, and it was from a quote by Dr. Davis, in which he said, referring to Adventists: “they strive to eat healthy.” I see this so often and I’m a grammar nerd. Use in this sense, healthy is a noun, cheese, or tomatoes, or meat, or vegetables. To eat a diet that his healthy is to eat “healthily.” Ergo, the Adventists strive to eat healthily.”
@David Mitchell: Health is a noun. Healthy is an adjective. Healthily is an adverb.
“Vegan” implies a moral component while “vegetarian” is mostly done for health reasons. I consider myself a vegetarian, but I also eat red meat, poultry, cheese, eggs, etc… I look at Vegans as people on a hunger strike…just doing it to get their point across.
Veganism doesn’t stop at food, they also don’t use animal-derived products, ie. leather, feathers, or fur.
I think the Vegan movement would be better served if they admitted their diet is not ideal, and were more transparent in their attempts to make an animal-free lifestyle as healthy as an omnivorous diet, for instance, overcoming a B-12 deficiency. They need to stop pretending that Veganism is “better” than other dietary choices.
I think that our livestock are treated poorly, and I applaud people who are bringing this to light. I protest in my own way; I buy only antibiotic and growth-hormone free meat, free range/grass fed when possible, harvested by me in the wild as much as possible. I do not see an ethical dilemma in the killing of animals for food, but I realize others are not as open to killing. There would probably be more Vegans if people had to kill their own lambs and calves and chickens. And even more if people visited feedlots and chicken factory farms. Animals are treated as a commodity and their health/healthfulness is not of primary concern to farm owners.
I wish Vegans well in finding a good, healthy diet just as I wish omnivores well. Both diets have their problems. A focus on whole foods needs to be the prime concern for everyone.
Can’t say it better myself!
“Vegan implies a moral component while vegetarian is mostly done for health reasons.”
That’s the strangest definition of these terms I have ever read. In reality, a vegan is someone who shuns ALL animal products (not just the flesh and organs, but also eggs and dairy), whereas vegetarian is a somewhat broader term that includes people who, in addition to plant foods, will also eat dairy, eggs or both. So the term vegetarian encompasses true vegans plus ovo-, lacto- and lacto-ovo vegetarians.
“I consider myself a vegetarian, but I also eat red meat”
Then you aren’t a vegetarian (neither am I, by the way). Saying “”I consider myself a vegetarian, but I also eat meat” is akin to saying “I consider the sky green.”
Great article Denise! And the longer, the better, when its the your quality writing!
Denise, this is the second time I’ve been to your website, and I want to commend you for your very rigorous treatment of these health topics. I have been a biochemist in health and longevity for 6 years now, and rarely do I find content so carefully considered.
I haven’t read your entire article above yet, but I wanted to stop and commend you. I learned something new at the part about humans having relatively small colons, and relatively large small intestines, for primates. I hear dietary comparisons to other primates quite frequently, and this is an important fallacy in that comparison – thank you!
Amazing, entertaining and unbelievably informative. Thanks so much for keeping up your brilliant work it really helps me in mine.
“a low-carb diet (the legit kind—5% of calories from carbohydrates)”
Sorry to pick on such a minor part of this long article, but why does a diet need to contain as little as 5% calories from carbs in order for it to be considered a “legit kind” of low-carb diet? In my book, that’s VERY low carb. In fact, I’d say 0-15% is VLC, and 15-30% is LC (approximately).
That’s a good question. A very good question, but there is an answer. The people who most benefit from a very low carb diet, and for whom this is really the only very good diet, are people who are severely insulin resistant or diabetic. They need it to be pretty low to gain the full benefit. I eat about 10% of my calories as carbs. Any more and I gain weight. For another person it could be more or less.
Well researched, easy to read, much needed review of the book Proteinaholic. Thanks Denise!
This is great – well researched. Just to add to the farmed fish points – at least with farmed fish, what happens has the POTENTIAL to be controlled, while with wild-caught, this potential is lost. Note the emphasis on potential – good management is required to produce good farmed fish. This is more of an issue of local or regional fish production, knowing what happens before you buy it, etc.
Reblogged this on Primal Nutritional Therapy and commented:
If you are going to buy a book today then buy Death by Food Pyramid and just read Denise’s critique of Proteinaholic here. You may want to skip to the ‘summing it up’ section unless you have a couple of hours to spare (it is worth a full read if you do have those couple of hours!)
Notice up to all satiety studies may be wrong on the satiety of fat because of the ubiquity of salt, which prevents fat being satiating.
http://suppversity.blogspot.com/2016/03/path-to-fat-induced-obesity-is.html
On this blog someone also posted link to a blog that mentions fat is problematic due to common taurine defficiency.
http://eatingoffthefoodgrid.blogspot.com/
So basically the satiety of fatty foods needs to be reevaluated in the context of very-low-salt, taurine-rich diet. Which is not a weird combination, but should be treated as default, as we want neither high blood pressure, nor a deficiency.
About CANCER and growth factors (IGF-1, mTOR etc.): one of the known facts about cancer is that it produces it’s own growth factors. It is even classified as one of the Hallmarks Of Cancer: “Self-sufficiency in growth signals”, and is followed by another “Insensitivity to anti-growth signals”.
So you cannot stop cancer by just lowering your intake of pro-growth foods. These may be able to speed up the development of cancer (adding external growth factors to internal ones), but avoiding them is not a cure, just a slowdown.
Studies on cancer-protected dwarf people may be misleading in this context, as such people have internal genetic problems in their cells with either being insensitive to IGF-1 at the cell level, or cells not being able to produce IGF-1. Cells that try to become cancer in such people inherit this legacy, and it makes difficult for them to become cancerous. Normal people have no such protection, internal growth factors production and sensititity is within capabilities of our cells.
Same with telomerase – cancers are self-sufficient in telomerase production, which prevents the stopping of cell replication (senescence) related to reaching the telomere limits.
Cancers are also automatically producing new mitochondria all the time without the need of external factors. Normal cells need something to increase mitochondrial number: PQQ (either a large dose supplement, or tiny doses found in food – on a purified chow with no PQQ rats die), excercise, low-carb high-fat diet etc. Cancer cells do this automatically.
In fact the newest breakthrough in cancer spread prevention (by Michael Lisanti, who previousy discovered Reverse Warburg Effect) is using antibiotics like doxycycline to specifically prevent new mitochondria from being formed. Opposite to what PQQ, HIIT excercise, or low-carb diet are doing. Normal cells are apparently able to survive this somehow (although people feel weak and sluggish them), while cancer stem cells have signitificant issues with inability to produce new mitochondria.
To add to the list of internal anabolic abilities of cancer: in cancer many of these overproduced mitochondria change their job from oxidation, to synthesis of substances. Including synthesis of substances like fat or cholestorol – as substrates for further cancer cell building. A powerful P53 anti-cancer gene does the following things:
– switches mitochondria to oxidation, away from synthesis
– this includes going from fat synthesis, to fat oxidation
– lowers glycolisiys, instead increases oxidation
– decreases retrotransposon activity
– the most known effect is that cells are more likely to commit suicide if genetic mutations are detected. For example elephants have this gene copied 20 times, and their cells are 2 times more likely to commit suicide after gene damage, than human cells. Mice with added copies of such gene get some anti-cancer protection, so maybe this is a valid candidate for a human genetic modification?
About substrates necessary for cancer: the bad news is that cancers can can get them from the neighbouring cells, rather than from external food. So again – eating substrates cancer likes can speed it up, but avoiding them won’t cure cancer, perhaps just slow it down. Cancer cells attack neighbourig fibroblasts with oxidative stress, this causes autophagy – self dissolution of fibroblasts. But the substances resulting from this dissolution of fibroblasts are utilized by cancer cells! Basically cancer eats the victim alive. It is so called Reverse Warburg Effect discovered by Michael Lisanti. You can fight it with strong antioxidants, or oxidation blockers, or autophagy blockers – he proposed NAC, L-NAME, Metformin, chloroquine. But MitoQ and MitoTempo mitochondrialy-targetted antioxidants were also found to limit cancer metastasis in research of other people. Notice that antioxidants are a mini-evil in the excercise industry, as they are known to prevent gains (are anti-anabolic), like muscle gains, from excercise.
Reverse Warburg Effect theory has strong consequences when it comes to energy: according to it both lactate and ketones (!) are a favorite food for cancer. Couple this with what we know about P53 driving fat beta-oxidation. And add the fact, that some cancer cells are “glutamine addicted”, and have problems without glutamine supply. Glutamine can be also produced by organism from glutamate – so both count.
To add to completnes: I’ve already written about P53 somehow slowing down transposons copying. The other known substances are anti-retroviral drugs called reverse transcriptase inhibitors. Since cancer mutations are in a large part driven by the increased transposon activity these may be helpful too. Transposon activity is increased with stress to the cells, a type of stress that goes above hormetic level. The stress may be caused by chemicals, like Benzo(a)pyrene, nickel, cadmium, mercury by oxidative stress (including one produced by cancer itself), radiation and so on.
A thought provoking commentary GTR. Would be interested in any references as to where you obtained this information.
As for general cancer anabolic, growth-loving qualities the evidence is like everywhere. Same with hallmarks of cancer. Telomeres are also described in multiple places. “P53 metabolism” is well established too.
The new stuff is more difficult to find. Some links:
1) Reverse Warburg Effect
https://en.wikipedia.org/wiki/Reverse_Warburg_effect
http://phys.org/news/2010-09-cancer-cells-alive.html
Other antioxidants:
http://www.science20.com/science_20/is_tumor_metastasis_prevention_on_the_horizon-142136
2) Transposons
http://www.anti-agingfirewalls.com/2015/11/12/transposable-dna-elements-part-1-basics-and-importancetransposable/
http://www.anti-agingfirewalls.com/2015/11/14/transposable-dna-elements-part-2-the-self-copy-machines-in-your-genes/
http://www.anti-agingfirewalls.com/2015/12/08/transposable-dna-elements-part-3-tes-and-and-other-key-mechanisms-of-evolution-incrnas-a-to-i-editing-alternative-splicing-and-exonization/
http://www.genengnews.com/gen-news-highlights/p53-maintains-genomic-stability-through-transposon-restraint/81252278/
http://www.pnas.org/content/107/46/19945.full
Click to access E89.full.pdf
http://nar.oxfordjournals.org/content/34/4/1196.full
3) Treating cancer with antibiotics via preventing mitochondria genesis
http://www.impactjournals.com/oncotarget/index.php?journal=oncotarget&op=view&page=article&path%5B%5D=3174
http://stemtektherapeutics.com/blog/cancer-stem-cells-mitochondria-antibiotics/
4) “cancer as a wound that never heals” and FN14 role in cachexia
http://www.latrobe.edu.au/news/articles/2015/release/major-discovery-into-cancer-weight-loss3
https://cosmosmagazine.com/life-sciences/how-stop-cancer-patients-wasting-away
http://phys.org/news/2005-05-cancer-exploits-body-wound-healing.html
http://www.medicinenet.com/script/main/art.asp?articlekey=26208
5) Human vs. animal genes for cancer
https://www.newscientist.com/article/dn28306-elephants-almost-never-get-cancer-thanks-to-multiple-gene-copies/
https://blogs.shu.edu/cancer/2015/10/14/why-do-elephants-have-lower-rates-of-cancer-than-humans/
Click to access 028522.full.pdf
http://phenomena.nationalgeographic.com/2013/10/23/humans-restrain-jumping-dna-that-chimps-allow-to-run-free/
http://arstechnica.com/science/2013/10/why-are-apes-more-genetically-diverse-than-we-are/
Compared to previous posts I feel obliged to:
1) Add some P53-metabolism related links, as these are the most revelant to the topic, and these are exactly the ones I have ommitted in the links spam.
2) Add some information on the role of antioxidants, as according to the newer data these (except perhaps mitochondria-targetted ones, like MitoQ antioxidants) may be harmful – increasing cancer spread.
The P53 anti-cancer gene is pretty much known about as the gene that protects DNA via vairous mechanisms, including turning on the defenses, or repair mechanisms, stopping the cell growth processes, while if the protection cannot be achieved – causes cell suicide. Majority of cancer cells that succeed either manage to silence this gene, or have a dysfunctional, mutated copy. Elephants with 20 times more copies of this gene than humans are well protected against such P53 problems.
It has a pretty long evolutionary history:
http://www.hypothesisjournal.com/?p=154
http://www.pnas.org/content/106/42/17609.full
http://www.science20.com/news_releases/p53_the_evolution_of_the_guardian_of_the_genome
Some of the mechanisms that it activates involve metabolism. Like decreasing glycolisis and glutaminolisis, while increasing oxidative burning of substrates. Or more generally – inhibiting anabolic processes in the cell, while increasing oxidative energy production; this is also about fats: decrease in fat synthesis, increase in fat burning. This also involves what mitochondria do: cancer cell try to turn them into anabolic, organic material producig factories, while P53 tries to turn them to energy production, thus getting rid of organic material.
So perhaps the type of metabolism that P53 promotes is the one that we can expect to be anti-cancer metabolism, while what it blocks we can expect to be pro-cancer metabolism?
http://www.cell.com/cell-metabolism/fulltext/S1550-4131%2813%2900289-1
http://cellandbioscience.biomedcentral.com/articles/10.1186/2045-3701-3-9
Click to access 1078-0432.CCR-11-3040.full.pdf
https://www.sciencedaily.com/releases/2014/11/141117110700.htm?
Going to antioxidants: one of the things you notice in the literature above is that P53 may need oxidative stress to activate the suicide of the cell.
(From the Cell link) “The regulation by p53 of carbohydrate and lipid metabolism is tightly linked to another important function of p53: the regulation of ROS. In its role as a “guardian of the cell,” p53 can eliminate the deleterious effects of oxidative insult either by limiting ROS damage in cells that can be salvaged or by using ROS to eliminate cells damaged beyond repair. Hence, if the insult is transient and repairable, then p53 can activate a suite of antioxidant responses, many of which are linked to carbohydrate or lipid metabolism. […] On the other hand, if the damage is irreparable, p53 may evoke a pro-oxidant state, which will ensure the demise of the damaged cell”
(From the cellandboioscience link) “Interestingly, in addition to the function of antioxidant defense, p53 can exert prooxidant function through transcriptional up-regulation of a group of prooxidant genes depending on the levels of oxidative stress that cells are facing (Figure 3). In response to severe oxidative stress, the intracellular levels of ROS are elevated, which activate p53, leading to the p53-mediated apoptosis and senescence to eliminate cells damaged by oxidative stress. At the same time, the activated p53 protein induces the expression of prooxidant genes, including PIG3, PIG6, FDXR, Bax, and Puma, all of which can further increase intracellular ROS levels and promote the p53-mediated apoptosis and senescence to maintain genomic integrity”
Getting too much conventional antioxidants on a constant basis, without this intelligence and adaptivity of controlling their levels based on context, may interfere with this process. There are studies of cancers that tend to quickly spread (skin cancers, lung cancers) that show conventional antioxidants (mitochondria-targetted antioxidants were not included) may increase the spead of spread – one of the mechanism being the inactivation of such P53 response.
http://www.scientificamerican.com/article/antioxidants-may-make-cancer-worse/
“Previous research has suggested that glutathione affects the activity of a protein called RhoA, which helps cells move to different parts of the body. “If you were to select one protein that is known to be involved in [cell] migration, RhoA is it,” Bergö explains. He and his colleagues confirmed that the extra glutathione in the treated mice caused levels of RhoA to increase in their metastatic tumors. In their 2014 lung cancer study they also found that antioxidant supplements caused lung tumor cells to turn off the activity of a well-known cancer-suppressing gene called p53; its inactivation is believed to drive metastasis. And Schafer’s work has shown that antioxidants help migrating breast cancer cells survive when they detach from the extracellular matrix, the network of proteins surrounding cells.”
In the below link shape of cancer cells is described – theo oval one, that facilitates mobility, and is prevalent with low oxidative stress – like with antioxidants, and the elongated one, that is stationary, and cells have it with some oxidative stress present.
http://gizmodo.com/antioxidants-might-actually-make-cancer-worse-1737510994
http://scienceblog.cancerresearchuk.org/2015/10/16/antioxidants-free-radicals-and-melanoma-spread-whats-going-on/
This cancer spreading process is rather complex than simple. Take for example the PI3K pathway which is thought to be enabler of cancer spread:
https://en.wikipedia.org/wiki/PI3K/AKT/mTOR_pathway
“The PI3K/AKT/mTOR pathway is an intracellular signaling pathway important in regulating the cell cycle. Therefore, it is directly related to cellular quiescence, proliferation, cancer, and longevity. […] There are many known factors that enhance the PI3K/AKT pathway including EGF, shh, IGF-1, insulin, and CaM. […] In many cancers, this pathway is overactive, thus reducing apoptosis and allowing proliferation. This pathway is necessary, however, to promote growth and proliferation over differentiation of adult stem cells, neural stem cells specifically. […] Additionally, this pathway has been found to be a necessary component in neural long term potentiation”.
So what happens when this overactive pathway in cancers is blocked in cancers? It looks like cell have a pre-programmed way to deal with such situation:
http://medicalxpress.com/news/2015-06-treatment-pi3k-inhibitors-cancers-aggressive.html
“Now, new research from scientists at The Wistar Institute shows that treatment with PI3K inhibitors alone may actually make a patient’s cancer even worse by promoting more aggressive tumor cell behavior and increasing the cancer’s potential of spreading to other organs.[…] The study showed that treatment with a PI3K inhibitor causes the mitochondria to migrate to the peripheral cytoskeleton of the tumor cells. While the mitochondria in untreated cells cluster around the cell’s nucleus, exposure of tumor cells to PI3K therapy causes the mitochondria to move to specialized regions of the cell’s membrane implicated in cell motility – meaning that the cell is able to move spontaneously – and invasion. In this “strategic” position, tumor mitochondria are ideally positioned to provide a concentrated source of energy to support an increase in cell migration and invasion.”
All this plastic, adaptive behavior of cancer cells cannot be a novel property of the cell, acquired through the new mutations. There’s no time for such evolution, and the behavior is too similar among completly separate cells, from different species. It is pretty well known that some behaviors of cancer, like the eternal growth, are related using genes normally used for other purposes, like embryonic development, or wound healing. But the self-defense and certain intelligence is not explainable by these. Some theories posit, that what we have in genes is a reservoir of heuristics acquired throughout our entire evolutionary history, and this includes heuristics (behaviors) of the time our ancestors were less differentiated, more loosely connected organisms, that fought hostile environment (cancer as a form of atavism). Other claim that this 8% viral DNA contents in our DNA has something to do with cancer behavior. Perhaps the overall genetic architecture is broken? Basically having a genetic bomb of things like persistent expotential growth in every cell DNA, just disabled as long as genes like P53 are active, when they fail – the bomb explodes.
Another molecule with complicated relation to cancer is hyaluronan (hyaluronic acid). On one hand it has been found to be a part of a diet of many longevity villages, where cancer incidence is very low, on the other hand there’s some evidence that it is related to cancer spreading fast. Young people naturally have a lot of hyaluronic acid, they tend to have low cancer incidence, but young-age cancers develop rapidly.
Somehow the same with IGF-1. It’s a growth factor, that increases cancer growth (in addition to hormones internally produced by cancer cells) but also a molecule that can make things younger. In fact one of the promising ways to reset the immune system intelligence via thymus regrowth. Notice you can do this by selectively treating only thymus with IGF-1.
Also people with large muscle deal better with cancer threat. Notice you can selectively increase IGF-1 in just muscles, rather than the entire organism with testosterone.
http://www.telegraph.co.uk/news/health/news/5371468/Men-with-big-muscles-cut-cancer-risk-by-40-per-cent.html
Same with HIIT excercise, that increases the number of mitochondria: it’s good to have some mitochodnria for oxidative burning, including efficient fat burning, as oxidative burning is anti-cancer. But the process of building new mitochondria itself is pro-cancer, as the cancer depends on building new mitochondria.
http://www.medicalnewstoday.com/articles/308325.php
So it looks like to overcome the adaptive behavior of cancers the strategies for decreasing cancers should also be reasonably adaptive? For example: if you don’t have cancer – build large muscles, increase mitochondria number, get younger with hyaluronan, or thymus regrowth. At the time you get bad markers, or learn about some cancer risk – immediately stop doing anabolic stuff, go catabolic, eg. use things like doxycycline to prevent formation of mitochondria.
Besides – for substances that might be potential cancer promoters – use only targetted versions, rather than whole-body ones. Eg. if you want to be an “enhanced” bodybuilder use testosterone, rather than growth hormones or insulin. If you want antioxidants – use only mitochondrially-tagetted ones. Use anabolic food mostly around workouts, and recovery time, rather than at every meal. And so on.
How many of your research reports that “debunk” Dr. Davis are sponsored by the meat, egg and dairy industries? With 2/3 of people in the US overweight or obese, record amount of Type 2 diabetes and hyper-tensions the real problem is not beans, rice or sweet potatoes.
It’s not meat or cream or milk either. It’s sugar and refined carbs like white flour. That plus, probably, too much omega-6, too little omeega-3 and too little vitamin D.
Paladin: There is an enormous body of original research sponsored by no one in industry going back at least to Yudkin (1963), and indeed, going back to Banting (170 or so years) linking excess carbohydrate consumption, particularly of dense, acellular carbohydrates with excess weight, and the biological mechanism is well known: it involves insulin resistance. What biological mechanism shows that fat in the diet becomes fat on the frame? And what body of research shows that consuming a high-fat, low-carb diet promotes overweight and obesity? Dr. Davis doesn’t appear to have come up with any. What do you have?
Like I said 2/3 obese or over weight in US is not from high carbs. Type 2 diabetes is not from our high carb diets. You can find your answer by going to your locale buffet.
An argument from eminence? From conjecture? From fondest hopes? From the desire to validate a dearly-cherished belief? What does “Like I said mean”? Because you said it, of course it must be true? By what metabolic pathways are fat and/or protein stored as fat? Science is fundamentally a process of evaluating evidence. An accumulation of confirmatory evidence lends credence to a hypothesis, but a single piece of contradictory evidence is sufficient to demolish it. There exists abundant evidence that reducing dietary carbohydrates and replacing them with protein and fat not only improves markers of metabolic health, but is the single best way to lose weight, regardless of the calorie consumption. What evidence contradicting this have you found, other than buffet behavior? Do you frequent them? What do people eat in such places?
I’ll make an argument based on USDA food availability data. The data from 1909 to 2010 for each macronutrient comes from this table
http://www.ers.usda.gov/media/179795/carbs_intake_d.html
And this underles the final graph in the following report.
http://www.ers.usda.gov/data-products/food-availability-(per-capita)-data-system/summary-findings.aspx
Using the 2010 numbers, digestable carbohydrate is 450 grams/day (1800 kcal), fat is 190 grams/day (1710 kcal), and protein is 120 grams/day (480 kcal). This gives macronutrient ratios of 45% carb/43% fat/12% protein.
This is almost exactly the composition of Cheetos. It’s not the fructose that’s made us fat since sweetener consumption is only up 6% since 1970. And no way it’s the steaks, with only 12% protein in the diet. It’s all the chips, which are composed of vegetable fat and refined starches (100% beta linked glucose).
If you believe that the fat in those chips won’t make you fat then go ahead and gorge on them. Like millions of other greasy chip consumers you’ll find out that fat is not a zero calorie substance.
THHQ: I truly don’t know what to make of your comment. I don’t eat chips, and I’m not fat. In fact, I don’t eat any sort of pseudo-food Nor do beliefs enter into how I think about food. Evidence is what counts. But I’m beyond the stage of thinking that macronutrient ratios have much relevance to dietary considerations. As Denise Minger, and many others, have pointed out, those ratios vary widely among healthy populations of people consuming traditional, non-industrial food. Nor is the question one of a single factor driving the obesity epidemic, as you imply (chips vs. fructose). It most assuredly is a complex of factors, including non-food environmental insults. I advocate eating mostly real food (meaning non-industrial food), with a particular emphasis on nutrient density and, personal experimentation to find what works best, since we are all a bit different. Giving up grains was a positive experiment for me, so I’ve kept it up. Substantially increasing vegetable consumption, especially wild greens, and seafood consumption, likewise, have led to improved health for me. By the way, Dr. Atkins wasn’t particularly young (70’s), and he didn’t die of anything diet-related. He slipped on the ice on the sidewalk, fell and hit his head, and slipped into a coma. His weight ballooned in the hospital from the consequences of this injury and the treatment for it.
All I can say Gary is that you are not an average American in how you eat and good for you.
Atkins massive edema is more typical of heart failure than the effect of a head injury. Since there was no autopsy we will never know a lot of things about how he died. My dad fell when he had a massive heart attack, but at age 88 he didn’t survive.
I think that obesity-wise it really is all in the chips. This USDA study identifies 80% of the increase in calorie consumption 1970-2005 as coming from added fats and refined carbohydrates.
Click to access eib33_1_.pdf
Not more fruit. Not more meat. Not more vegetables. Not more dairy. And only a marginal increase in added sugars – pastry, candy and the dreaded Big Gulp. The efforts of Lustig/Taubes/Ludwig are directed at the wrong target. Too much time wasted sniping at a small increase in fructose rather than the major factors. I’m cynical enough to believe that Big Chip wants it that way. Take the attention off the added fat with “science” and make people believe that Cheetos won’t make you fat.
THHQ: Good to know that we are substantially on the same page. Alas, how true that most don’t know what real food is any more. It is because we are a nation of sheep, anesthetized by TV, technology, and a misplaced trust in mommy-government. Curse George McGovern and Ancel Keys, a true charlatan. This is how the medical industry has been able to carry out the statin scam for so long.
I’m getting tired of hearing the argument against citing anecdotal N=1 evidence on various diet/health proponents who died young, from Atkins to Pritikin to Adelle Davis. IMO it IS significant that Colonel Sanders outlived all of them and IT WAS NO ACCIDENT. Living a long and healthy life is a lot more than macronutrient tweaking. Longevity is multifactorial.
Recently I found someone who did something useful that demonstrates this. I found Dr. Perls work. Through the magic of statistics, he has transformed Boston University’s centenarian study into a user-friendly working model. You fill out a health profile, of the type used in any Dr’s office for new patients, and the model projects a life expectancy. It also gives you a laundry list of thing you can change to increase longevity, along with the expected effect. For instance, f I quit eating my daily pastry I’ll live 1.5 years longer.
https://livingto100.com
So far I’ve been using the model for various what-if’s:
-If I continue living the way I’m living I will live to 90, and could push that to 95 by cutting out those pastries among other things. My dad lived to 88, so it’s in the ballpark of possibility.
-If I change to the Atkins/HFLC/Taubes/Teicholz diet (sedentary, high LDL, max red meat), and all my other parameters remain constant, I will live to 87.
-If I plug in Dr. Atkins published parameters, a 73 year lifespan is projected…within 1 year of actual…
-If I plug in Ancel Keys published and unpublished parameters, a 99 year lifespan is projected…within 1 year of actual…
Thanks for the excellent post! You mean “the excess protein gets converted into glucose (via gluconeogenesis).” Right!
Whether less or more protein, presumably the body converts all it into glucose very slowly comparing to the carbs so there is no insulin spike to transfer quickly the energy into the fat cells.
When I eat low carb but high fat the body (liver) will finally would convert it (or part of it) to glucose from the fat. What is the difference of metabolism in high fat or high protein relating gluconeogenesis?
Would a high fat result in a faster weight/body fat loss or a high protein (both cases low carb)?
Delivered in true Denise style 🙂 “Extraordinary claims require extraordinary evidence.” Indeed.
FYI for those following this post who are interested in the evolution of the discussion between Ms Minger and Dr Davis, we’ve posted a response to this blog post at Proteinaholic.com: http://proteinaholic.com/a-response-to-denise-minger-part-1/
I appreciate the commenters who are following the lead of the two protagonists in this scientific debate by seeking truth with respect and humility.
– Howard Jacobson, PhD, contributing author to Proteinaholic, by Garth Davis, MD, and Whole: Rethinking the Science of Nutrition, by T. Colin Campbelll, PhD (as well as books on digital marketing strategy that would probably make you yawn)
According to Wikipedia entry on an example hunter gatherer tribe (Ache people):
“Systematic recording of dietary intake while living in the forest entirely off wild foods suggests that about 80% of the energy in the diet comes from meat, 10% from palm starch and hearts, 10% from insect larva and honey, and 1% from fruits.”
“Most important (in descending order) are nine-banded armadillo, paca, South American tapir, capuchin monkey, white-lipped peccary, South American coati, red brocket, and tegu lizards.”
What would the prediction of your theory be about the effects of such a diet?
I read the generally derogatory things that you and the Dr have to say about Denise. I have only bought one diet book in the last year and that was Keys Eat Well and Stay Well. A certain amount of protein needs to be replaced every day. Beyond that it’s just calories, albeit expensive. Keys said it all. Nothing more needs to be said.
I applaud Denise’s efforts to move us away from the unproductive macronutrient wars. Your book is stereotypical and I won’t be buying it. If in future you launch all-out war on salty fatty starchy snack foods I give you my wholehearted support. That’s where the obesity problem lies IMO.
Of possible interest–overfeeding on higher protein intake results in less fat, more muscle (vs lower protein intake):
http://www.ncbi.nlm.nih.gov/pubmed/27159194?dopt=Abstract
Oh, lovely post! I esp. loved the kudos for fish! When I look at populations (both today and back when) … the fish-eaters … and esp. the shellfish eaters … tend to be the healthiest. Wheat/mammal eaters (often the same peoples: the ones that live inland) tend to be the least healthy. I do get frustrated with authors that dump “animal protein” all together in one category. And “grains” together too.
The people promoting veganism tend do lump all animal protein together though. There are some issues with red meat (as you pointed out quite well). But the studies on fish eaters all seem to show that fish eaters are both smarter (better brains!) and healthier. Even when there is more mercury in their hair or nails. Shellfish (scallops, mussels, squid, etc.) might be even more awesome, and they are a food that can be raised with little environmental impact.
In terms of Omega 3 … they are experimenting with azolla as fish food. It is a small floating plant, which happens to be high in Omega 3. And protein. And fish love it. Easy to grow in shallow ponds, and it has the side-effect of killing mosquitoes. I grow quite a bit of it, and feed the extra to the chickens. I don’t grow fish myself, so I grow the azolla mainly to kill the mosquitoes, and this is the 2nd year where I’ve had zero mosquito bites! But the idea that “farm grown fish” has to be high in Omega 6 … I expect that using grains as fish food will eventually go away. There are cheaper ways to feed fish, and they result in higher-quality fish.
Anyway, glad to see you back!
Selenium is protective against mercury toxicity, rendering mercury in seafood largely a non-issue. The Bristol study is behind a paywall, but it clearly shows that children of mothers who eat seafood are smarter and healthier. The growing fetal brain requires large amounts of DHA, depleting the mother’s stores. And what do doctors tell pregnant women? Don’t eat fish. Go figure.
Hi heather twist, I agree. A good example, is the pre European Maori who ate lots of the abundant seafood – fish and shellfish, and small birds, as well as kumera and fern root as the main carbs. The early Europeans noted their tall stature, good teeth and bearing, and general healthfulness. And they were very resourceful and smart, as evidenced by their ability to outwit the English in battle.
Good basis for a book,
I’d really like a resource I can lend people that is definitive and accessible
I can log in with FB, but where’s the link to share on FB?
For lack of a better recent place to put this, I’ll post it here.
From time to time, the topic of Keys’ cherry picking the Seven Countries comes up, usually with the accusation that the rationale for selecting the countries was not explained. The rationale is clearly stated here:
“The countries included in the study were Yugoslavia, Italy, Greece, Finland, the Netherlands, the United States, and Japan. Why were these particular countries chosen? Yugoslavia offered coastal and inland populations with vegetable fat versus animal fat diets. Italy represented a prototypical Mediterranean lifestyle, with a diet full of grains, pasta, legumes, fruits and vegetables, olive oil, bread, and wine. Greece provided a setting with very high
dietary fat intake, principally in the form of olive oil, but very little saturated fat. Finland had an exceptionally fit population, but high rates of heart disease, and a diet extremely high in saturated fat. The Netherlands represented a European population with an intermediate dietary pattern, with meat, butter, and tuberous vegetables. The United States component consisted of railroad workers, originally chosen to study the effects of different activity levels on heart disease, but then incorporated into the Seven Countries Study because the participants tended to remain in one place over time, making follow-up relatively simple. Finally, Japan was chosen as representing a lifestyle with minimal dietary fat intake.”
Seven Countries was focused on fat consumption, but it was much broader than a controlled ward study. Countries (and within countries many sub-populations) were selected to see the effects of diet and lifestyle on multiple health outcomes, not just CVD rates. In the Japanese section, for instance, it is interesting to read the observations on stomach cancer in a very high carbohydrate diet.
Click to access keys_yusuf_article.pdf
Denise is my hero and has saved me from my vegan rabbit hole that left me with permanent peripheral neuropathy. Thank you Denise!!
Christy: This is a similar condition to what statins did to Dr. Duane Graveline (spacedoc). I agree, Denise is first rate.
There’s some issues with the protein oxidation (PROTOX), which depends on the processing method – the more processing (like grounding), higher temperature, higher pressure, or the longer processing time (like aging meat) causes more protein oxidation.
Both hunter-gatherer habits or Chinese style of eating freshly-killed meat prevent protein oxidation related to time elapse.
Eg.
http://onlinelibrary.wiley.com/doi/10.1111/1541-4337.12127/full
I started Paleo and later keto in 2011. Since then, I have found that the best diet for me, is the one you write in your conclusion: lots and lots of veggies (some of it raw), some meat with most of it being wild fish/oysters, some legumes/rice (once a week each or so). Basically, I now eat seafood 3 times a week, and land meat once a week (usually Sundays). It’s the way my Greek ancestors ate too: mostly veggies, some meat. Maybe that’s why the “Mediterranean diet” was so good: because it had those things in that ratio. Plus, their old style wheat was always properly fermented (although I don’t eat any grain except rice, since I can’t tolerate them).
Studies have shown that hunter-gatherers ate a diet of about 70% vegetable matter. It wasn’t meat, meat, meat every day all day long. Eat your veggies kids and lots of them.
Is there a good overview of high temperature cooking vs lower temperature cooking methods?
Is there any good source that goes over high temperature vs low temperature cooking?
Hello, Miss Denise!
I have two questions for you. It is not a loaded question, although it may seem so. I really want to know your answer, no strings attached.
Can you order these raw food items, putting first the more dangerous?
a) raw soy beans
b) raw wheat seeds
c) raw alfalfa sprouts
d) raw chicken eggs
e) raw goat eyes
f) raw cow milk
g) raw mealworm larvae
h) raw apple
A follow up question. After proper cooking, the danger of these foods decreases. Does the order change too?
Boy, everybody thinks they have the answer to longevity don’t they. Fact of the matter is…everybody dies. Get a life.
the 44-month study on diabetes that you so gleefully link to shows that all of the patients on the low carb diet remained morbidly obese after 44 months, with weight loss slowing down significantly after the first three. I hope people reading this blog have the presence of mind to double check your claims
Excellent read. I feel somewhat vindicated being an athletic omnivore who practices intermittent fasting.
RE: RDAs. Dr Garth appears to be right here and Ms Denise Minger appears to misunderstand the concept of RDA. Individual minimum protein requirements are a random variable, hence they cannot be represented by a single number, rather by a statistical distribution. when Dr garth writes that RDAs are optimum values, actually he means ‘safe values’. RDAs are not minimum values, RDAs are points on the statistical distribution of minimum requirements, more precisely thy are high-percentile values representative of a safe or optimal conditions where most individuals (97.5%) are safe from starvation. The single values which make up the statistical distribution are minimum requirements. RDA= Reccomended daily allowance, not Minimum daily allowances. According to the WHO’s 2002 report, RDA= optimal or safe or reccomended value is 0.83 grams proteins per kg ideal weight per day, whereas modal or more frequent minimum requirement is 0.63 grams proteins per kg ideal weight per day.
So Denise, you make your reputation (including getting a contract for a book deal from a Paleo-food publisher no less) by pissing on the idea that eating fruits and vegetables is healthy for people. But you in fact eat mostly vegetarian and eat meat only once every few years? The Paleo-food industry, of which you are now a paid member, claim loudly that meat is the best thing a person can eat. But if meat is so incredibly good for you, then why on earth are you eating meat only once every few years? Are you kidding? You don’t see the hypocrisy of that?
Either you actually didn’t read any of Denise’s input, or you’re making a strawman argument, or you have limited understanding abilites. Denise fully advocates a plant-based diet.
I’ve been reading John Yudkin’s popular diet book This Slimming Business from 1958. He presents a highly cogent argument for a mixed diet which is relatively low in added sugars and starchy foods:
“Bread and cheese, milk and rice pudding, meat and potatoes; these are combinations of foods which have very sound nutritional backing as well as being gastronomically desirable.”
And regarding CVD:
“This is not the place to argue it all out in detail, but I am certain that the best way of preventing coronary disease is not to be overweight, and not to become too sedentary. Get on your feet, do more physically, keep your weight down – that is my advice.”
This is the voice of the man who launched the HFLC movement. His diet restricts starchy and sugary carbs using a counting system and tables (5 gram units, called CU’s, and limited to 15 CU’s per day or 75 grams). His system is very similar to the ADA carb counting system for diabetics. Unfortunately Atkins, Taubes, Eades and Lustig skipped over most of what their well-educated and respected predecessor said. They dumbed down his precise counting system in favor of banned food lists. And they left out the essential part about exercise.
Finally they all deemphasize calories-in-calories-out, which Yudkin repeats over and over:
“The irrefutable, unarguable fact is that overweight comes from taking in more Calories than you need.”
“One thing is absolutely certain. There is no secret about weight control. You must lose weight if you take in fewer Calories than you put out. So far no one has ever found a single exception to this rule. If you can bring me an example where it is not true, I am prepared to be convinced. But it is about as likely as showing me an example of apples rising up from the ground into trees. Newton’s law of gravitation is no more certain than the laws of conservation of mass and of energy.”
While Yudkin believed that sugars and starches trigger overeating, he never bans them, only restricts them. He didn’t hold the HFLC belief that fat has a magic advantage over other macronutrients.
New information comes out and intelligent people change direction, foods have a different thermogenic effect, that’s why Atkins, Taubes, Eades and Lustig skipped over most of what their well-educated and respected predecessor said.
A simple question to you: have you ever submitted and or published a paper in a peer reviewed journal on nutrition and or medicine about your findings and criticisms. If no could you explain why ?
Ahhh using simple intelligence and persistent checking of sources is not enough for you ?
Thank you SO MUCH for writing this article. I just watched “What the Health” last night and was enraged with the cherry picking and manipulation. This article really spells out each individual point very nicely (Although I am aware of most of this info, it’s nice to see it all put together in one place to re-read)
Did it occur to you in creating this review that the author was sloppy or purposefully misleading. I tend to towards the later because of the types of errors you cite.
Please note that some of the errors cited by Denise Mingers are not errors. For example, the #1 ‘inaccuracy’ on RDA. Denise Minger gets it all wrong. She should be more careful on statistics 101. RDA, as the first reference cited by her clearly states, is a 97.5% percentile of the minimum requirement. Such an high percentile means that’s an optimum, or safe value, among the distribution of minimum requirements. If it sounds confusing, please go and study statistics 101: probability distribution functions, normal distribution. Also please study the main references on protein RDA like the WHO publications, which examines the metanalysis from Rand.
Now, the RDA might be too much of a low safe level in some conditions, but that’s another issue. Dr Garth Davis is not wrong at all in his book.
Thank you for the article. I will be avoiding the Proteinaholic book for sure.
For me, the big problem with a lot of these fear-mongering food books such as Proteinaholic is that they are written for general average audiences who typically get no exercise to speak of, or perhaps only moderate exercise at best. The nutritional needs of serious athletes are much different, especially in the strength-based fields of powerlifting, Olympic weightlifting, bodybuilding, etc.
I lift hundreds of pounds of weights multiple times a week, and for people like me it is absolutely essential to keep protein intake high for proper muscle recovery and growth. Meat, eggs, dairy, and fish serve this purpose extremely well.
Actually, there are a few vegan strongmen who appear to do reasonably well on plant-based protein (Patrik Baboumian, Kendrick Farris…). I agree that many vegan athletes are best in endurance sports rather than in strength sports. Unfortunately, strength sports is a field on its own since it is governed by PED (performance enhancing drugs), so we are no more into a natural metabolic environment and the rules on protein consumption are different.
Theoretically, plant based protein is about the same as animal protein (barring some EAAs proportions), whereas a +10% amount should be calculated on the requirements with respect to animal protein because of the fibery matrix.
Another aspect is that vegan strength athletes are pretty few. Bottom line, most considerations in proteinaholic are sensible and not faraway. The author does not consider strength athletes as far as I remember.
Denise, and many other, I see you as ‘academic exercise coaches’. All this dietary stuff is very much revealed by our own bodies. I’ve been through the bad experiences you’ve been through beginning in the teen years and into the twenties,… and even into the thirties,… and with continued refinements through my 40’s.
I’ll be brief here,…. but, from what I find, animal flesh (usually cooked, if not always), bovine milk products (preferably raw, but not always) (Goat milk is not sufficient for me as a staple food), fresh fruit, greens (mainly asteraceae and apiaceae), good beer,… and minimally of everything else,…. which means infrequently or rarely eating starch,…. keeps me really healthy. All in moderation of course. Consuming to perform in life, and not for custom or ‘being social’ (though yes, I realize sometimes one may have to do so). Also, avoiding leguminosae foods I find is best for me, even Inga edulis, which is ‘Ice Cream’, eaten raw,…. although if eaten when they’re yellow-ripe, that may be acceptable, but not necessarily, so I just avoid it,… they’re most enjoyably eatable in the green-with-some yellow phase of development, – more moist, not so dry as when yellow (I include this a more detailed point). On that matter even Carob may not be prime,… as with other Leguminosae.
Also, another example, chocolate, as in chocolate bars, even 90% chocolate, can clog lymph veins just as partially hydrogenated (I know) or fully hydrogenated (I guess) vegetable oils can.
Best wishes,… but I swear the dietary field is in huge disarray because of making it way too complex along with the very unnecessary ‘scientific’ studies,… which are mostly a waste of time, by far.
Our bodies reveal, get in tune.
You look like Anais Nin.
I have read so many books on diet. Paleo, Keto, high-carb low-fat and vice-versa and just read your entire post straight through in (two hours?) with a few side trips to review the footnotes, and I am confused to the point of exhaustion. In all the reading I’ve done I have seen the same studies used to support their diet, and claims by the authors insisting that the studies were misrepresented, cherry-picked or certain data was simply not included (as in The Seven (Six?) Country Study. I’ve read your post on that also. I am approaching food these days with one eyebrow raised in suspicion, and my refrigerator sits in the corner and leers at me. I recently purchased your book from Amazon and am waiting for it to be delivered. I am impressed with your apparently non-biased research and I am hoping to get some real answers.
Sandra: We are whole human beings. The nutrients we derive from good quality foods is only part of what gives us health. Mental health is just as important. I follow a few simple rules about eating: 1. Enjoy your food, and eat in the presence of others whenever possible. 2. Eat the best quality food you can afford. 3. Avoid what Dr. Price called “the displacing foods of modern commerce,” flour, sugar, vegetable oils, and canned foods. It is possible to have vibrant health on a carnivore diet, on a vegetarian diet, and a whole bunch of others (but not vegan). Most important of these is #1. Enjoy food, enjoy life, and don’t worry about anything.