Long time no blog, fam!
So, I had this hope that the next thing I posted here would be a grand explanation about my extended absence, all the weird stuff that’s happened over the past few years, my loss of faith in nutrition as a front-line approach to healing, and various other sundries I’ve been storing up in my brain-attic.
But then COVID-19 happened, and if that isn’t the biggest cosmic plan-changer that ever did plan-change, then I don’t know what is. So we’re gonna roll with it. And at the risk of writing something that’ll already be outdated by the time I hit publish (such is the nature of current events), I’m hoping this post will stay evergreen (or at least ever-chartreuse) by sheer virtue of its universal core theme: navigating conflicting, emotionally charged narratives in which objectivity behooves us but doesn’t come easy.
So LET US BEGIN.
In case you didn’t notice, the cyber-world (and its 3D counterpart, I assume, but we’re not allowed to venture there anymore) is currently a hot mess of Who and what do we believe? This is zero percent surprising. Official agencies have handled COVID-19 with the all grace of a three-legged elephant—waffling between the virus being under control/not under control/OMG millions dead/wait no 60,000/let’s pack the churches on Easter!/naw, lockdown-til-August/face masks do nothing/face masks do something, but healthcare workers need them more/FACE MASKS FOR EVERY FACE RIGHT NOW PLEASE AND THANK YOU/oh no a tiger got the ‘rona!; on and on. It’s dizzying. Maddening. The opposite of confidence-instilling. And as a very predictable result, guerrilla journalism has grown to fill the void left by those who’ve failed to tell us, with any believability, what’s going on.
“Twitter these days.” (Source)
Exercising our investigative rights is usually a good thing. You guys know me. I’m all about questioning established narratives and digging into the forces that crafted them. It’s literally my life. Good things happen when we flex our thinking muscle, and nothing we’re told should be immune to scrutiny.
But there’s a shadow side here, too—what I’ll henceforth refer to as “lopsided skepticism.” This is what happens when we question established narratives… but not the non-established ones. More specifically, when we go so hog wild ripping apart The Official Story that we somehow have no skepticism left over for all the new stuff we’re replacing it with.
And that, my friends, is exactly what’s happening right now.
I’ve been watching homegrown theories about COVID-19 spiral through various social platforms, born from a mix of data (sometimes) and theory (usually) and anecdote (always). They’re generally a pushback against the mainstream narrative about the coronavirus’s timeline, severity, concern-worthiness, fatality rate, treatment, infection breadth, classification guidelines, origin… round and round we go. Some theories are reasonable (“Has the virus been here longer than we think?”), some are untenable (“The ‘virus’ is actually radiation poisoning from 5G towers!”), and many more lie somewhere between.
Most importantly, they all have one thing in common: a tendency to embrace any and all supportive data without, well, making sure it’s true.
Y’all know what I’m talking about. Evidence we’d never give the time of day if it didn’t work in our favor. The “I remember reading somewhere…”, the “I have a friend who knows someone who…”, YouTube interviews that are impossible to fact-check (but please just trust this person’s top-secret info from an organization they can’t name without the Feds beating down their door), crowdsourced anecdotes, retracted papers, retweeted screenshots of Facebook comments from people whose names and profile pictures are blacked out, the whole shebang.
This stuff. Is. EVERYWHERE.
Unfortunately, throwing a bunch of really bad evidence together can create the illusion of a well-supported theory. And this is what’s happening, my dudes. This is what it’s come to. In our rabid quest to undermine the Powers That Be and figure out what’s really going on, we’ve thrown quality control out the window and become that which we loathe: loyalists to narrative over data.

Case in point, let’s look at what might be the most popular COVID-19 theory circulating right now: that mortality stats are getting padded by assigning deaths to COVID-19 that are really from other causes—thereby making this whole thing seem worse than it actually is. Depending on the sub-theory, this might be due to financial incentives for hospitals (more COVID-19 patients = more $$$); a coordinated government hoax to trick people into relinquishing their sovereignty; a way to butter us up for mass ID microchipping; something something lizard people; and so on.
And from what I’ve seen—and by all means correct me if I’m missing something—this theory draws on the following claims:
- The CDC has literally issued guidelines telling doctors and medical examiners to classify deaths as COVID-19 if they “presume” the patient has it—no test results needed.
- CDC data shows a precipitous drop in pneumonia deaths right around the same time COVID-19 became a thing—suggesting pneumonia deaths have been getting reclassified as COVID-19 deaths, and creating the illusion of a pandemic.
- People who die with coronavirus, but not from coronavirus, are getting counted as COVID-19 deaths—again inflating the body count.
- Despite COVID-19 mortality skyrocketing, total mortality is staying the same (or even dropping)—suggesting a “cause of death” shuffle, if you will, and betraying the idea that we’re seeing additional deaths from a new disease. (Alternatively: “Only people with preexisting medical conditions are dying and they were gonna keel over any minute anyhow.”)
This theory would be pretty awful if it’s true. We’d have been got. Duped. Manipulated AF. But how solid is the evidence? Have we actually peeled this thing apart piece by piece before getting all ragey about the injustice of it all?
Oh, we haven’t? Well GUESS WHAT WE’RE GOING TO DO NOW?
Let the unpeeling commence.
Claim #1
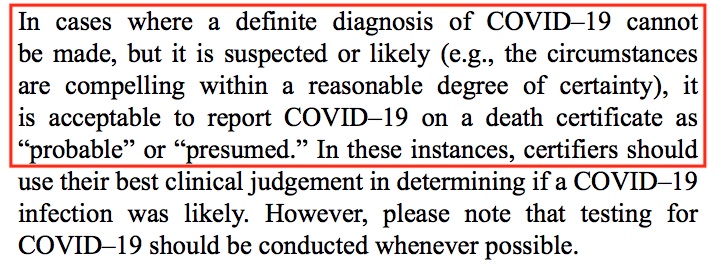
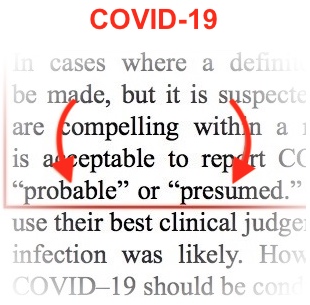
1. First, the whole “CDC is telling people to report COVID-19 deaths without testing!” ordeal. The damning bits come from the CDC’s COVID-19 reporting guide (PDF), which gives permission to use COVID-19 on a death certificate if it’s “suspected or likely” and “‘probable’ or ‘presumed'”:
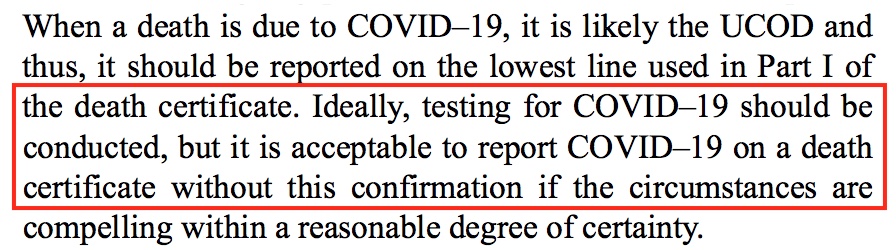
And also says it’s okay to report COVID-19 without testing confirmation:
And the WHO’s “Emergency use ICD codes for COVID-19 disease outbreak” gives a whole death code for COVID-19 cases that aren’t confirmed via test:

And finally, this National Vital Statistics System document says COVID-19 can be put on a death certificate when it’s “assumed” to have caused death:

The point of contention here, which has sparked something of an outrage in important places such as Twitter, is that these guidelines allow a level of guesswork that could mess things up real bad. Especially if there’s already some sort of incentive to bend data in the direction of more coronavirus deaths. What if people assign COVID-19 willy nilly to anyone who has a cough or fever? Or who had a poorly-timed bout of allergies? Where does the line get drawn? For sure, “probable,” “presumed,” “suspected,” and “likely” aren’t very reassuring words when it comes to a disease we’ve shut down the whole globe to contain.
But is this actually conspiracy worthy? And, in a clinical setting, with actual doctors doing doctor things rather than us internet-dwelling oafs imagining how it all might go, would these guidelines really lead to a significant over-reporting of COVID-19 deaths?
For starters, let’s look more closely at that CDC reporting guide. Although it does say COVID-19 deaths can be assigned without a positive test result, it also emphasizes the importance of drawing from all available evidence in order to make an informed judgment:

And it turns out, this is really no sketchier than the CDC’s guidelines for certifying pretty much any cause of death. Seriously. According to the agency’s Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting (PDF), it’s okay to use personal “judgment” when there’s uncertainty:

And yes, medical examiners and coroners are invited to give their “opinion”:

So are physicians, according to the CDC’s Physician’s Handbook on Medical Certification of Death—note also the use of “probable”:

And medical examiners are broadly allowed to list “causes that are suspected,” and to “use words such as ‘probable’ or ‘presumed'”—again, for any death-cause:

And here we see the CDC’s Instructions for Completing the Cause-of-Death Section of the Death Certificate telling us again that a condition can be listed as “probable” even if there isn’t a definitive diagnosis (and also the words YOUR and OPINION written in CAPS because the CDC successfully learned how to yell on the internet; good job, CDC):

*I know it’s tiny; click for bigger
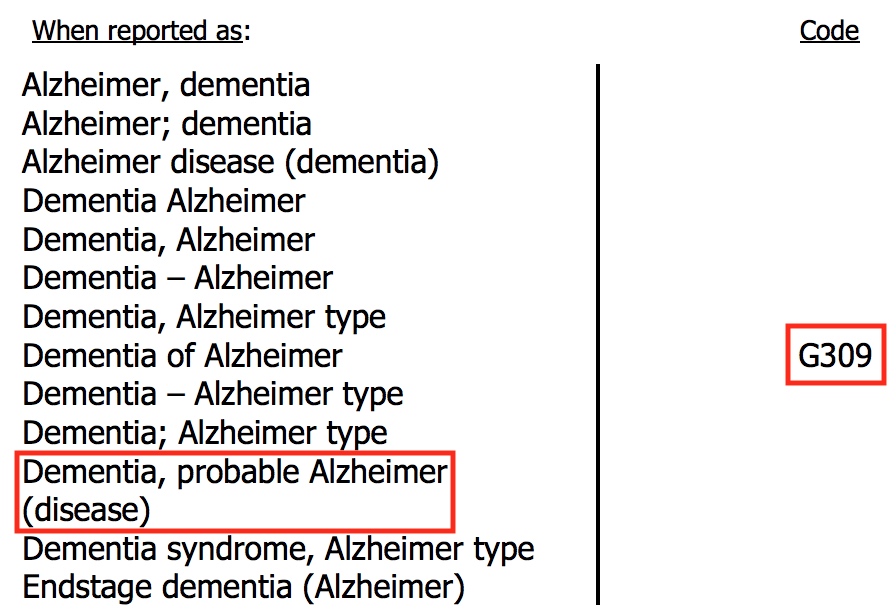
Are you sick of this yet? Guess what? Alzheimer’s deaths can get the same code whether the disease is confirmed or “probable”:
Oh hey, remember 83 seconds ago when we were so mad that COVID-19 deaths could be listed as “probable” or “presumed”? Because it seemed like some unique-to-coronavirus word twist intended to help pad the death stats? REMEMBER?
No. Just no. This same language is consistent through all the cause of death guidelines, no matter the killer in question. It’s been that way for years. And COVID-19 is even lucky enough to get separate codes for “probable” versus “confirmed” cases, which is more than we can say for some other diseases. (And to boot, some places were already seeing COVID-19 mortality explode before reporting the “probable” deaths at all.) Heck, the guidelines for coronavirus deaths are far more straightforward than the maze-like estimation formula the CDC takes for flu mortality.
In short—and please make me eat my words if I’ve overlooked something important here—this really isn’t outrage-worthy. Certifying any form of death is an imperfect, partly subjective process, and concessions for that reality are baked into all sorts of official guidelines. If overzealous COVIDing is happening (and you’re welcome to investigate any theory-offshoots that it is), it’s not because the CDC told death certifiers to cook the books.
Claim #2
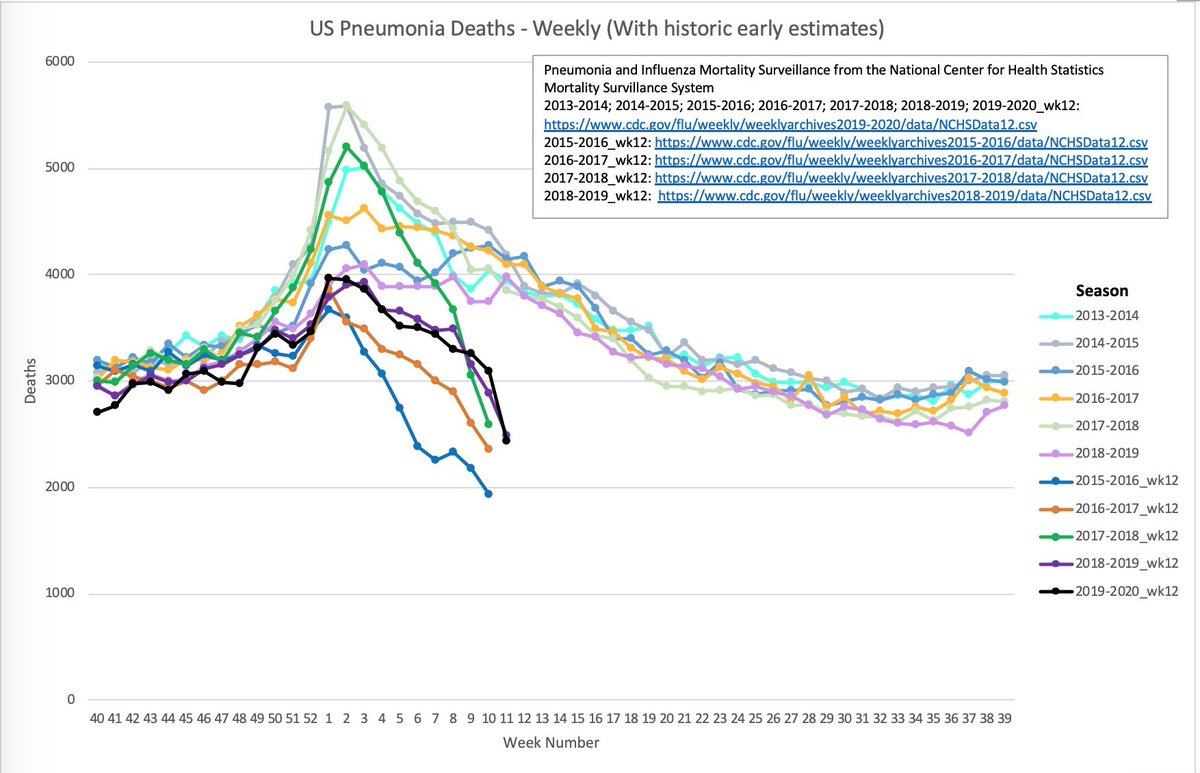
2. As for pneumonia deaths getting classified as COVID-19 deaths? This graph of CDC data has been making the rounds as evidence that something very shady, very shady indeed, is going on. As you can see, around week 10 of this year (starting March 2nd), pneumonia mortality told its wife it loved her and then jumped off a cliff:

If we’re already primed to think the COVID-19 numbers are being doctored, we might take this graph at face value and add it to our stash of outrage fodder. But that would not be smart, friends. Face value is where critical thinking goes to die. And so, in the spirit of questioning literally everything, we must ask: could anything else explain what we’re seeing?
As a matter of fact, yes! So much yes! We only have to venture as far as the CDC’s Provisional Death Counts for Coronavirus Disease (COVID-19) page to see what’s up. Go take a look. Especially the “Delays in reporting” section. Thar be some gold.
Basically, the CDC’s death-certificate-processing system is a slow, laborious beast that ensures any recent mortality data is always incomplete. They give a decent rundown of how death certificates get handled from start to finish:
Provisional counts of deaths are underestimated relative to final counts. This is due to the many steps involved in reporting death certificate data. When a death occurs, a certifier (e.g. physician, medical examiner or coroner) will complete the death certificate with the underlying cause of death and any contributing causes of death. In some cases, laboratory tests or autopsy results may be required to determine the cause of death. Completed death certificate are sent to the state vital records office and then to NCHS for cause of death coding.
And here we have a special shoutout to our favorite infectious diseases, noting that pneumonia, flu, and COVID-19 certificates take extra long to trickle into the data pool due to manual coding (emphases mine):
At NCHS, about 80% of deaths are automatically processed and coded within seconds, but 20% of deaths need to manually coded, or coded by a person. Deaths involving certain conditions such as influenza and pneumonia are more likely to require manual coding than other causes of death. Furthermore, all deaths with COVID-19 are manually coded. Death certificates are typically manually coded within 7 days of receipt, although the coding delay can grow if there is a large increase in the number of deaths. As a result, underestimation of the number of deaths may be greater for certain causes of death than others.
Zooming in even further, the CDC gives some stats conveying just how incomplete their recent data is, and boy howdy is it a sorry sight. At any given moment, data from two weeks ago is likely to be barely over a quarter complete, while data from eight weeks ago is still less than three-quarters complete:
Previous analyses of provisional data completeness from 2015 suggested that mortality data is approximately 27% complete within 2 weeks, 54% complete within 4 weeks, and at least 75% complete within 8 weeks of when the death occurred. Pneumonia deaths are 26% complete within 2 weeks, 52% complete within 4 weeks, and 72% complete within 8 weeks (unpublished). Data timeliness has improved in recent years, and current timeliness is likely higher than published rates.
The CDC even slaps this little disclaimer after each table of COVID-19, pneumonia, and flu death counts:

Once again, with feeling: CDC mortality figures are initially very incomplete, low-balled-as-all-get-out, and retroactively fill in over time. Which means a weird pneumonia death-drop will show up any time we check the most recent data, COVID or No-vid.
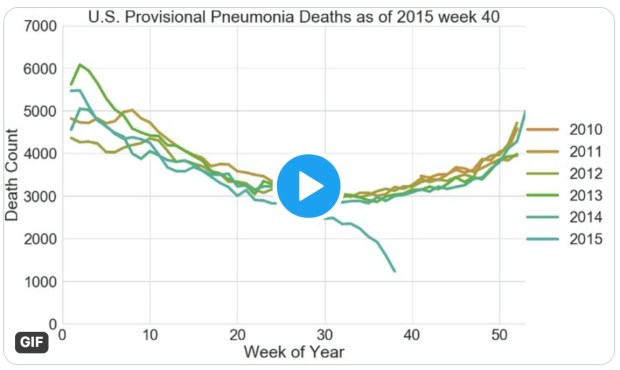
To illustrate, Joseph Dunn graphed the CDC’s pneumonia data as it appeared on the same mid-March week of each year since 2013. Behold:
Look at all them swan dives!
And data scientist Tyler Morgan even went to the trouble of graphing the data from every weekly CDC pneumonia report published in the last decade, to show how the lines shift as data gets back-filled. Click here or on the image below for the really cool animation (it’s weirdly beautiful and absolutely worth the 30 seconds of your life):
In other words, there’s nothing anomalous at all about 2020’s pneumonia trends. Nothing. The popular graph up top is a meaningless piece of hooey and it’s sad that it went viral.
Note: there’s an issue here I’m cognizant of, but intentionally not touching on yet, which is that some people believe the CDC (and any other government organization) literally makes up data from thin air, thus rendering all of the above irrelevant. This level of conspiracy is beyond the scope of this post, but I may try to address it at some point later on. Not from a data angle, but from a psychological one.
Claim #3
3. Here we have the wildly popular claim that people are dying with COVID-19, not really from COVID-19. At least, not in the numbers we’re being told. It’s basically a steroided-up version of Claim #1—just with more trickery and plot-thickness and finger-tenting.

The evidence for this one is a lot harder to fact-check, because there are actually no facts to check. Its trueness rests on us believing that doctors and death-certifiers are being marionetted by evil forces and/or just plumb don’t know what they’re doing.
The closest thing we’ve got to “evidence” are citationless social media statements like the above, which we’re expected to trust because LOOK AT ALL THOSE RETWEETS!, a few well-publicized examples of allegedly mis-assigned COVID-19 deaths, and Youtube interviews with people who are pretty sure they know what’s going on. Like this one, featuring Dr. Annie Bukacek, with nearly 750,000 views at the time of writing.
Apparently, she knows her stuff. And the stuff she knows is that the coronavirus figures are being manipulated!

Hmmm…
Hmmmmmm…



Hmmmmmmmmm.
Serious question: how many of us bothered to look Dr. Bukacek up before thrusting her atop a pedestal of trustworthiness? And sharing her video far across the lands? And assuming she’s an impartial commentator on the whole situation (her praiseful introducer was literally her pastor)? Should we really put faith in someone we didn’t even know existed ten seconds ago just because 1) they’re telling us what we want to hear and 2) an internet headline made them sound prestigious?
By the way, to state the obvious, this is me intentionally and very shamelessly cherry-picking to make a point. Not all of her reviews are bad. Nor do the existing ones necessarily prove she isn’t credible. And if we wanted to be truly fair, we could prod deeper and ask whether she might be getting bad-review-bombed due to her vocal pro-life activism or religious affiliation or anti-vaccine stance (she’s definitely got some haterz). There’s a lot of sticky tricky gray-zone business in evaluating reputation, which is why—whenever possible—we should investigate a person’s claims rather than their character.
But the issue here is that with Dr. Bukacek, we can’t “investigate her claims” without installing cameras into every death certifier’s brain and watching what unfolds within their basal ganglias. So we’re left with only her word. And one person’s word is not useful data. Even if it’s the best of persons and the best of words.
Now, to play devil’s advocate with my own arguments here, there’s another popular video—this one featuring Coronavirus Response Coordinator Deborah Birx—that seems more genuinely suspect. I saved this one for last because it might actually have some merit. In it, Dr. Birx talks about the USA’s “very liberal approach to mortality” and outright states that people who die with COVID-19 are counted as COVID-19 deaths:
Transcript: There are other countries that if you had a preexisting condition, and let’s say the virus caused you to go to the ICU and then have a heart or kidney problem, some countries are recording that as a heart issue or a kidney issue and not a COVID-19 death. Right now we’re still recording it and we’ll—I mean the great thing about having forms that come in and a form that has the ability to mark it as COVID-19 infection, the intent is right now that those—if someone dies with COVID-19 we are counting that [as a COVID-19 death].
It’s not surprising this clip went gangbusters! It seems like a deal-clinching A-ha for anyone who suspected COVID-19 was getting slapped onto every death possible.
However, here and always, context matters. After all, this segment was carefully cropped from a much longer coronavirus briefing from April 7th. And if we listen to the full segment—the audience question that came before this clip, and the follow-up question that came after it, and the follow-up answer Dr. Birx gave, and the addendum answer Dr. Anthony Fauci gave—we can better orient ourselves in the conversation that was happening.
Go have a listen. The relevant stuff starts at the 1:39:07 mark:
Could it be that Dr. Birx thought the question-asker was wondering if lack of testing might cause under-reporting, and tried to reassure her by explaining that the current COVID hotspots are flush with tests? And that people with “heart or kidney problems” wouldn’t be reported as dying from those things if they’d ended up in the ICU from coronavirus? (Especially given that COVID-19 itself can cause cardiac injury and kidney damage?)
It sounds to me like the thrust of the asker’s question—which was more along the lines of “Are we sure we’re not over-counting deaths?!”—went over the heads of the task force, and they addressed a different issue than the one she was trying to get at.
But I can’t read minds. And I can’t prove that it’s not all just political doublespeak and of course they understood the question. And I think there’s far too little information in this video alone to assess it from a “scam vs. not-scam” angle. And most importantly, in the absence of actual mortality data that could clue us in to potential over-reporting, I doubt analyzing this thing to smithereens can bring us any closer to the truth.
But, you be the judge. And speaking of mortality data…
Claim #4
4. Lastly and not leastly: the claim that COVID-19 isn’t actually causing excess mortality; we’re just reshuffling death causes to stack up higher for COVID-19 and lower for everything else. Boom, insta-pandemic!
First, a note. This is a Very Important claim. It’s the supreme ruler of all the claims that came before it and perhaps all those incipient ones that will come after. It has executive power and a VIP card for entry into the most highly guarded chambers of our brains. This is because, unlike causes of death, actual body counts can’t be fudged. This is the one true test. If COVID-19 really is taking lives en masse above and beyond what we’d expect from normal death trends, total mortality is where it’ll show up. If it’s not, then our game of death-code musical chairs will be revealed for the con that it is.
Again: Very Important claim. This is the crux of it, my dear readers.
Fortunately, there’s an easy way to test this claim: looking at total mortality trends in areas that COVID-19 has purportedly ravaged, and comparing that to historical mortality in the same location. An absence of anomalous death spikes—taking into account, of course, delays in processing death certificates and the lag time between infection and dying—would suggest we’re over-reporting COVID-19. And if excess mortality does appear, then we either have to concede that COVID-19 isn’t a nothingburger after all, or propose that some other ghastly, unnamed entity is stealing lives very coincidentally at the same time we have a made-up pandemic.
*Keep in mind, too, that our current near-global quarantine should slash deaths from accidents and certain crimes and infectious disease—and thus “normal” mortality rates for right now would likely be lower than for previous years.
So let’s dig into this. The “COVID-19 is overblown” theory asserts that total mortality isn’t doing anything unusual. At least not significantly so. No more than a bad flu year, let’s say. And depending on the source, we may be furnished with graphs that seem to demonstrate this truth to our hungry, data-seeking eyes, such as the following for England and Wales:

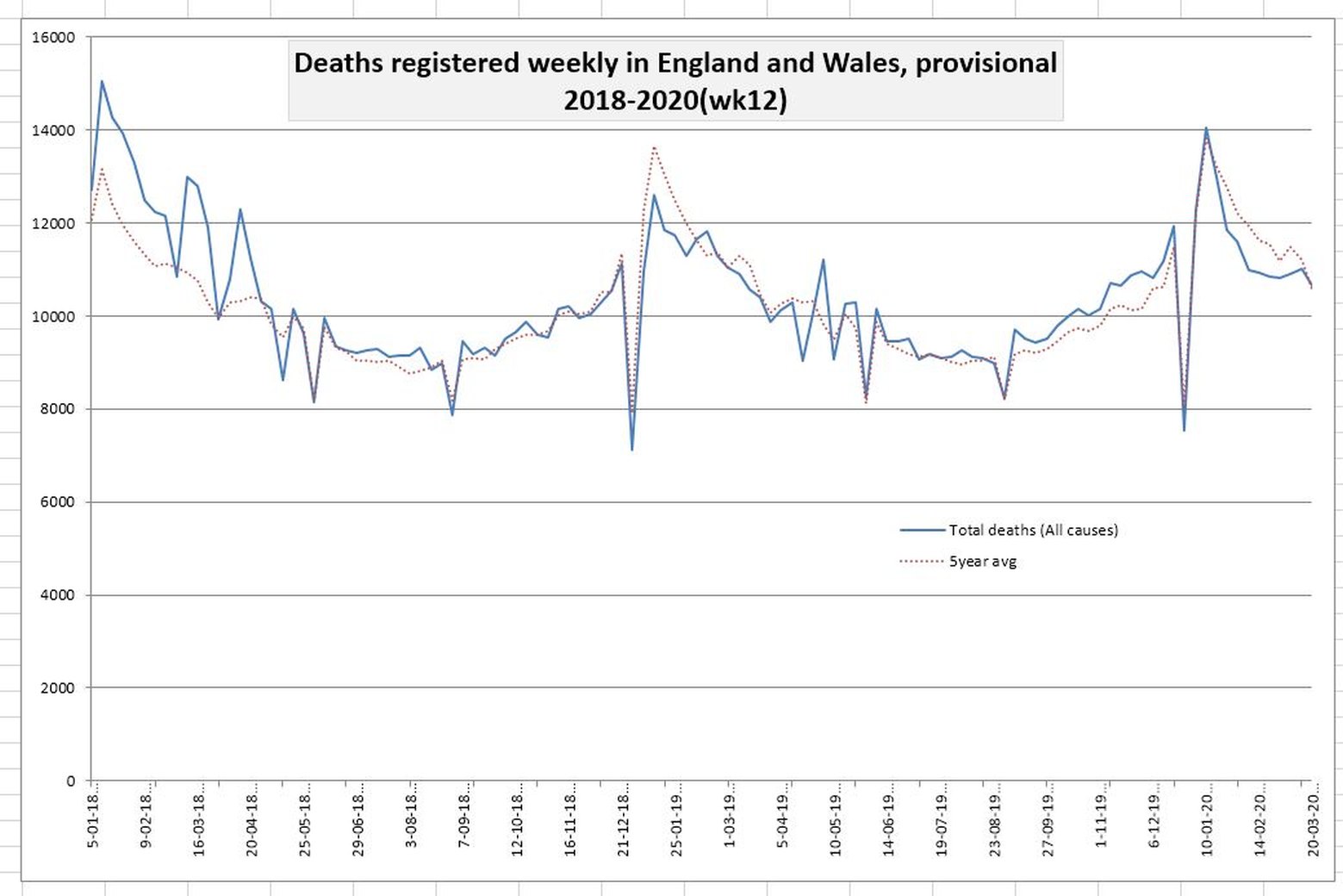
There’s one very big problem here. Check the dates.
Almost universally, the “See, it’s nothing!” graphs use data from mid to late March, when COVID-19 was just starting to pick up steam in the areas it’s most recently terrorized. And in March, there really weren’t massive mortality spikes, except perhaps for Italy. Nothing to see here, folks was true. And no one in the infectious disease world was claiming otherwise. In March, the rumblings of upcoming mortality explosions was what people were getting worried about, not the numbers as they then stood. The whole deal with “exponential growth” is that it’s—wait for it—exponential. This is how we went from 0 reported COVID-19 deaths in the USA on February 15th, 65 deaths one month later, and 30,000 deaths yet another month later.
So let’s see what happens when we look, instead, at more recent data from countries with known COVID-19 outbreaks. (This site is a great starting resource for raw mortality data and some visuals.)
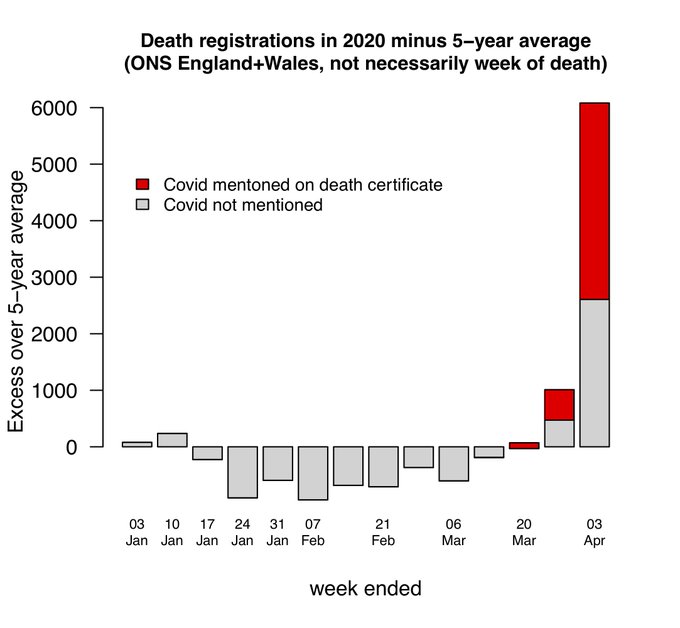
First, here’s what’s up with England and Wales now (source):

And another depiction suggesting COVID-19 deaths may be under-reported (data source and image source):
London, OMG (source):

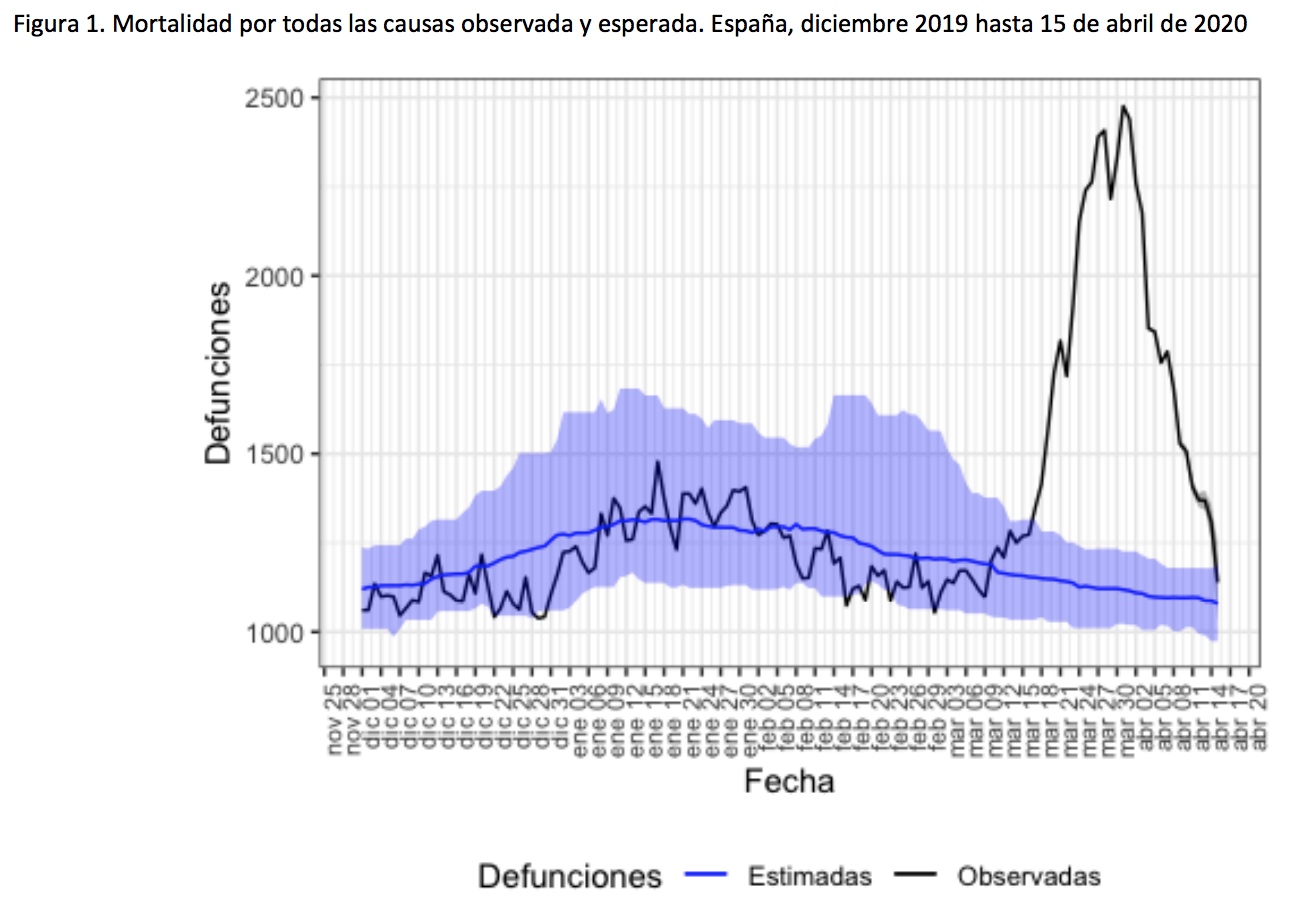
Excess mortality in Spain as a whole, from December 2019 to April 15 of this year (source):
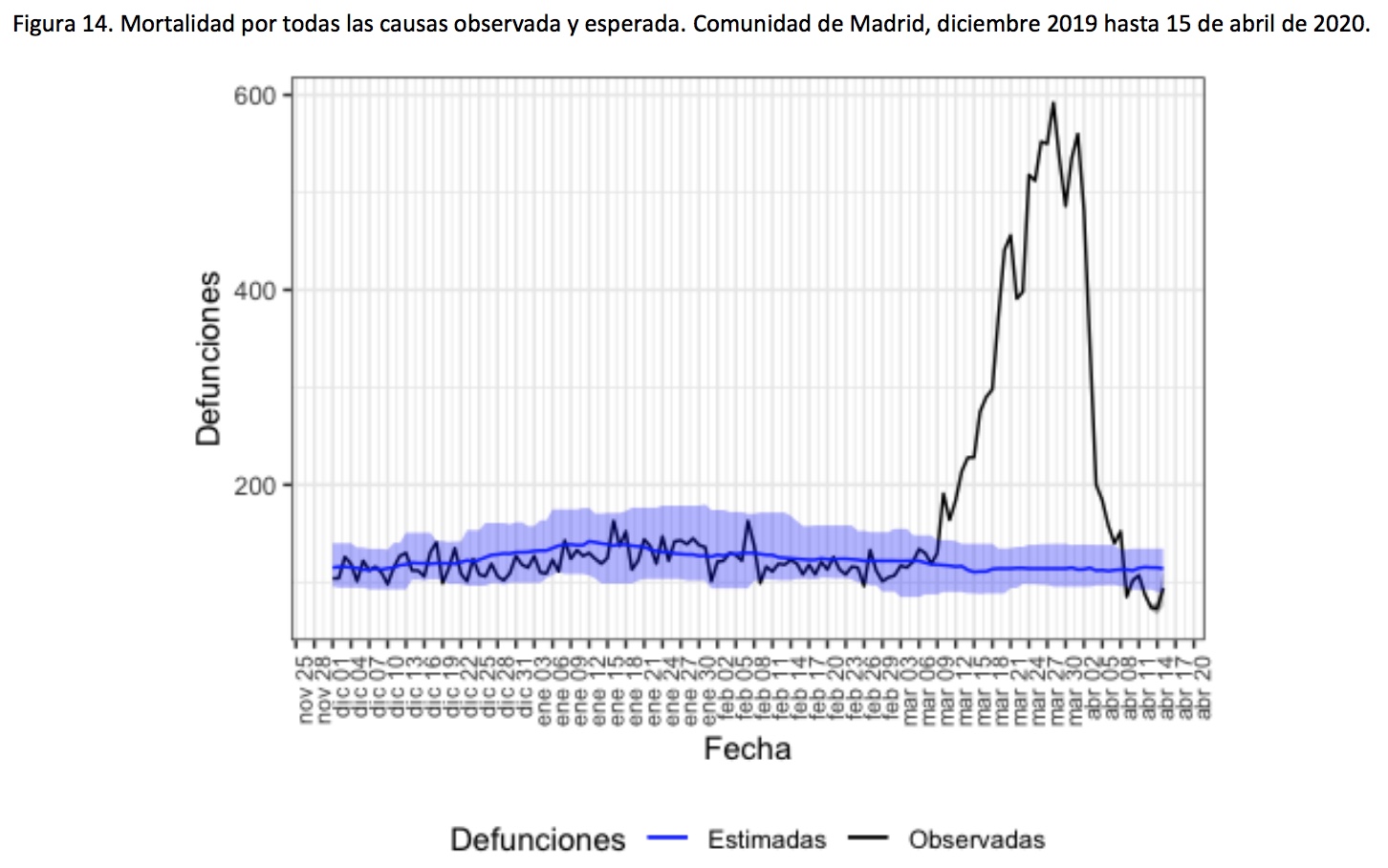
Madrid, in particular, got clobbered:
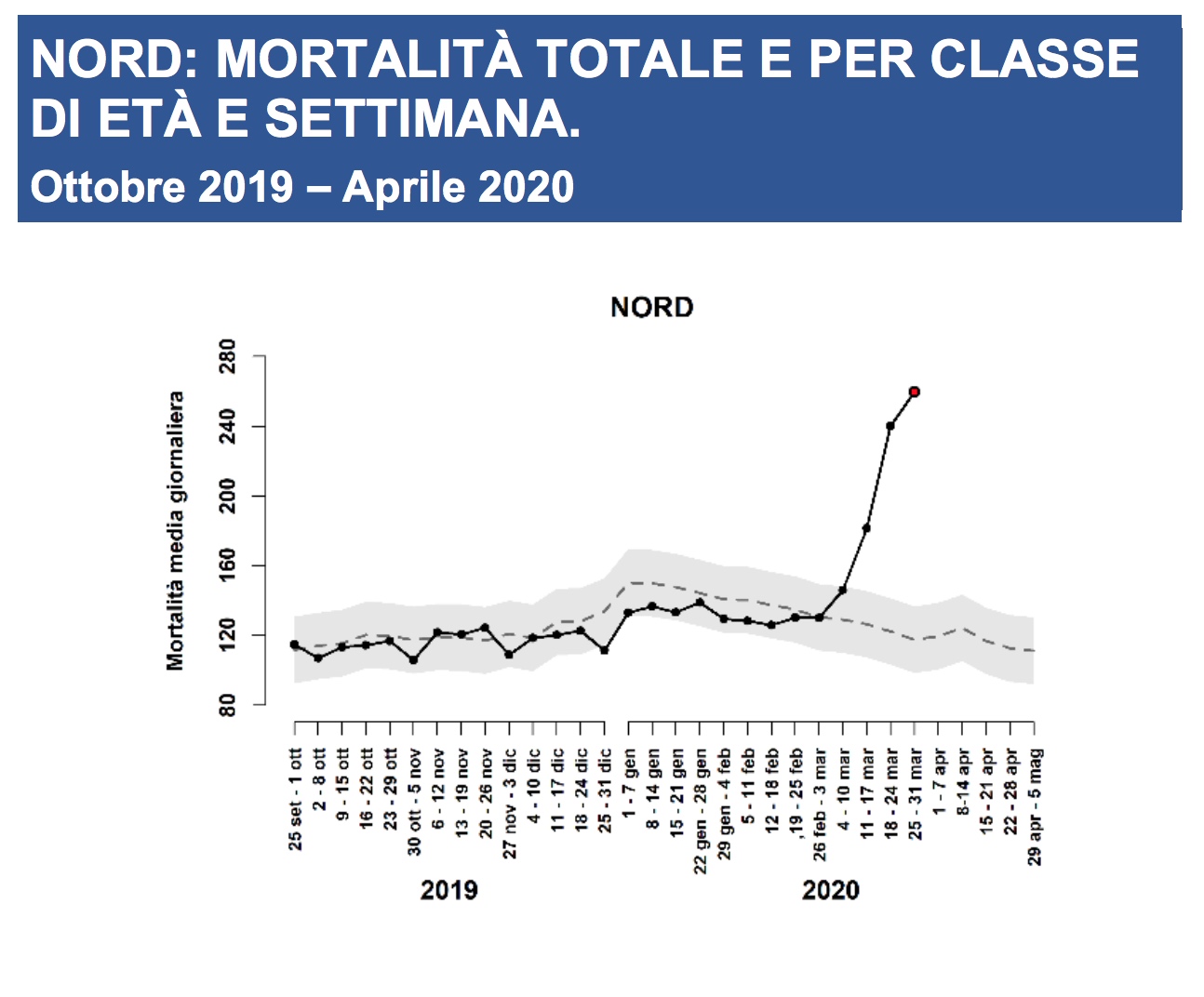
And Bergamo, Italy, in which March deaths far surpassed anything seen locally within the past decade (source):

Heck, northern Italy as a whole (source):
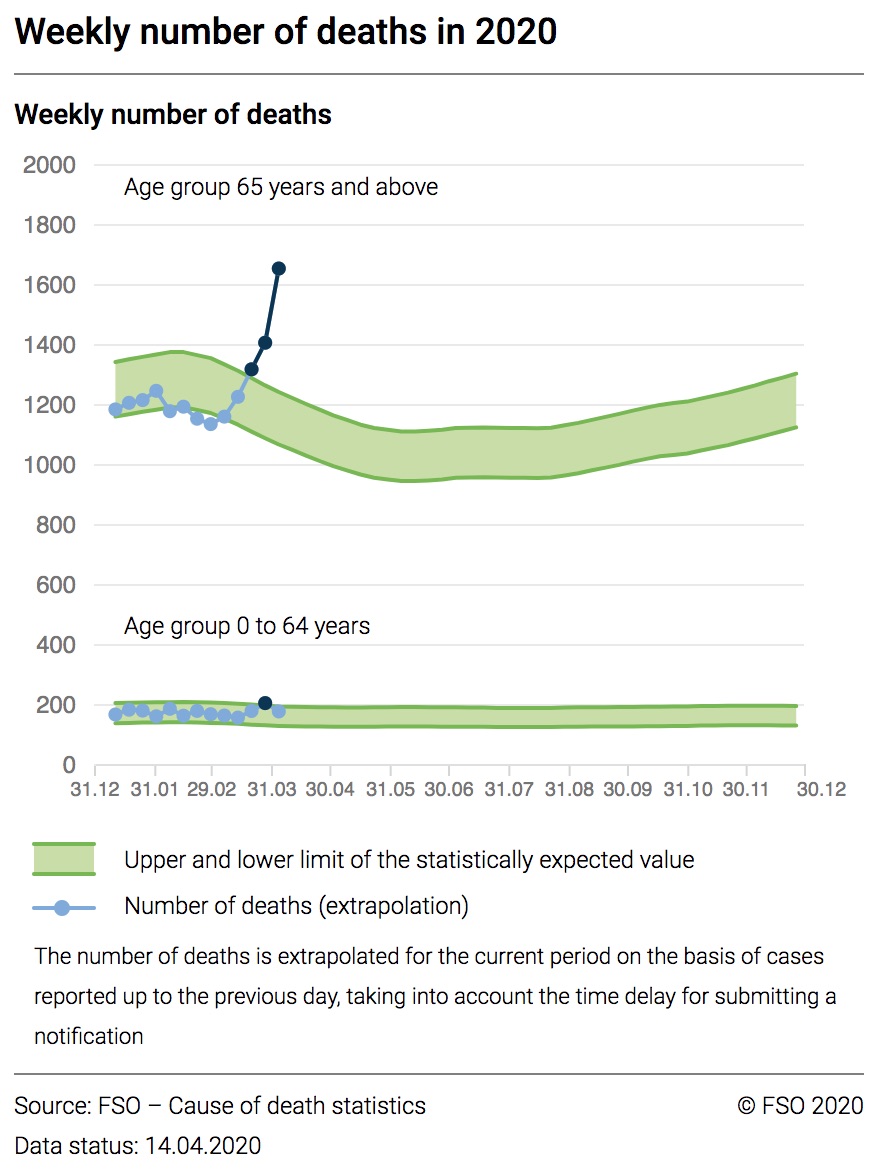
Switzerland looking pretty wonky for the 65-and-olders (source):
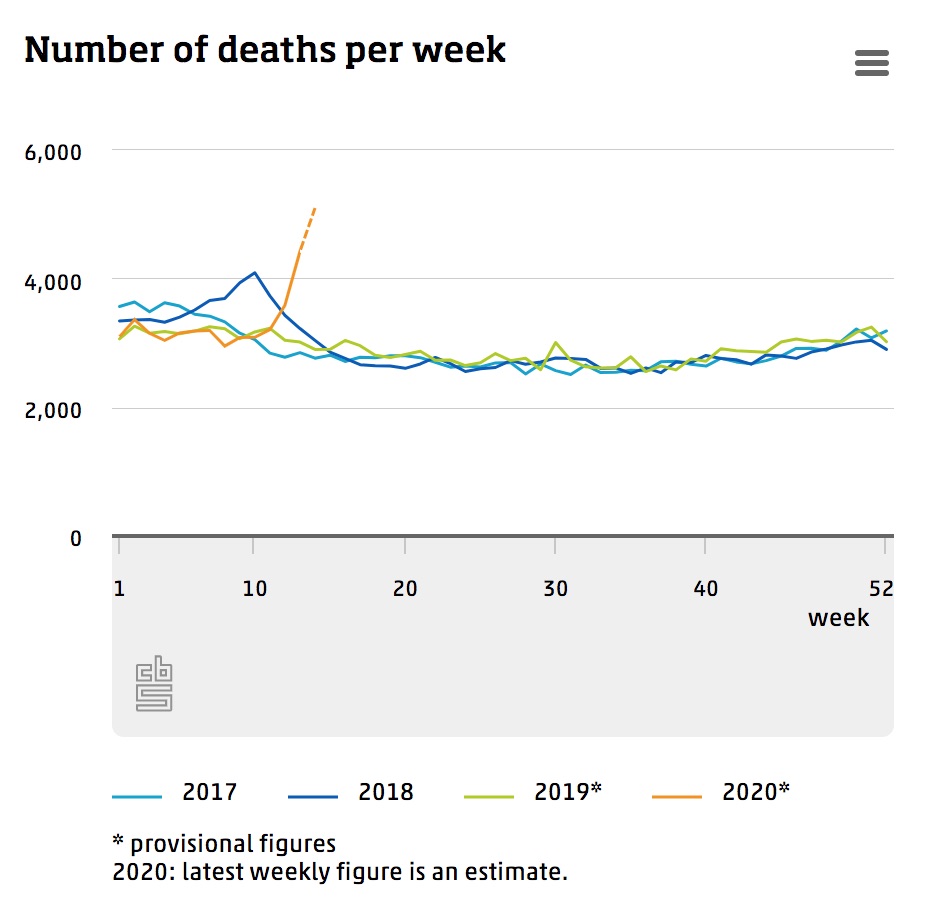
Total mortality in the Netherlands (source):
A big chunk o’ Europe getting excess-mortalitied (source):
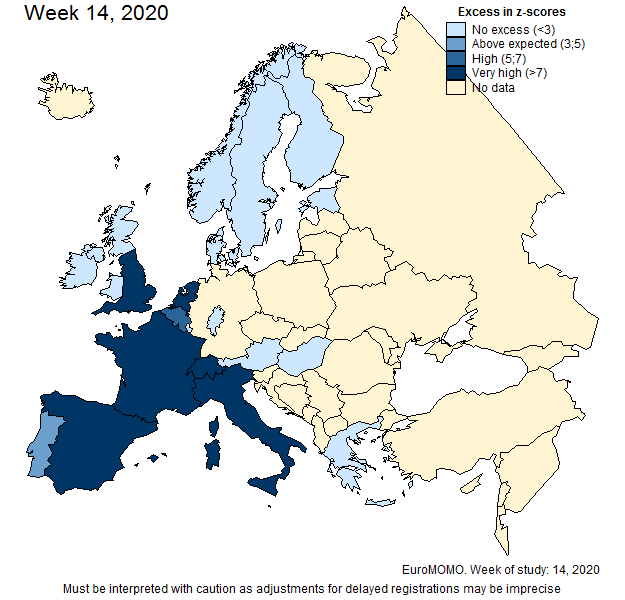
Note: the EuroMOMO site (which produced this image) is great for tracking excess mortality in Europe, but right now, it’s only useful on Thursdays when it’s updated before becoming functionally irrelevant for the next six days.
New York City, graphed by the New York Times (article here; viewable with free subscription) (NOTE: this data is almost two weeks outdated and the the April deaths are now many magnitudes higher):
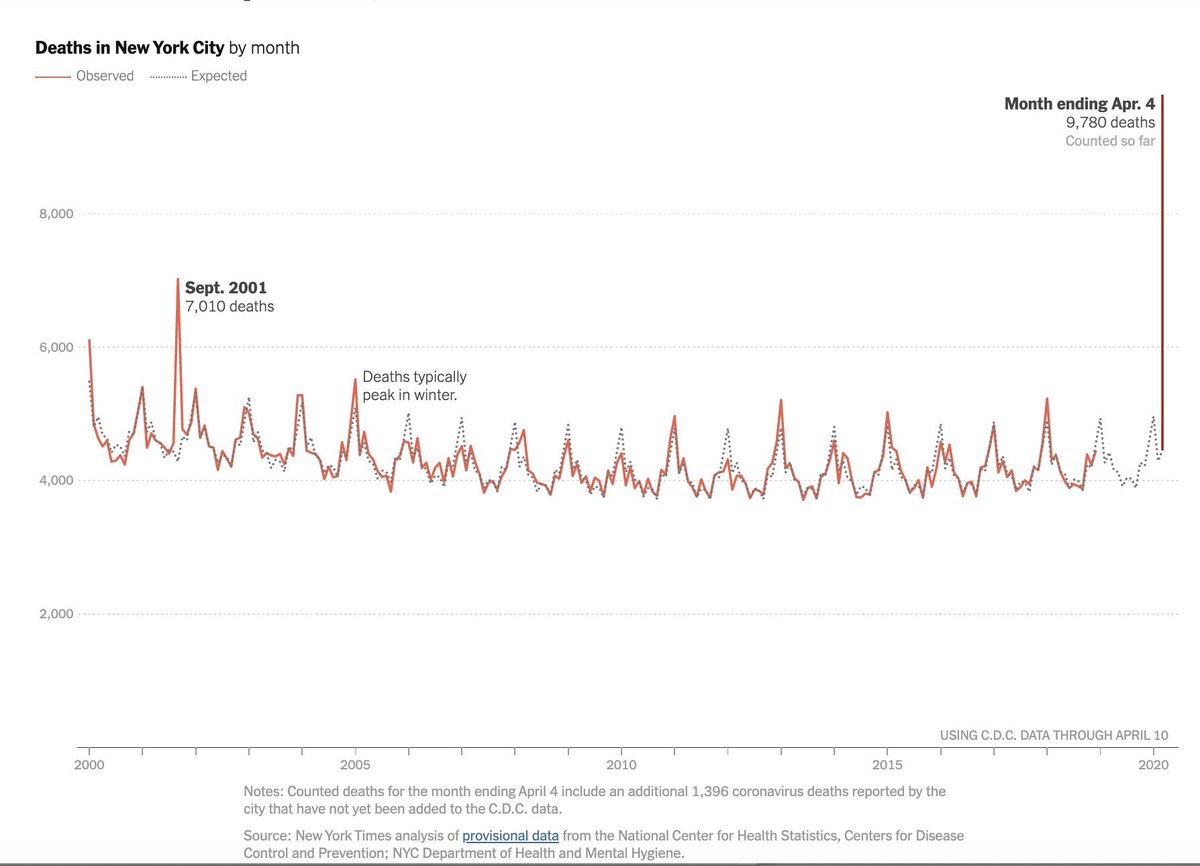
We could do this all day, but you get the point.
Here’s the deal, folks. People. Are. Dying. The mortality trends for COVID-19-affected areas look like what happens when you’re trying to draw a straight line and then sneeze. This is not normal. This is not how things “should” look. We can argue all we want about how accurate the COVID-19-specific data is—and indeed, there’s plenty to argue about— but total mortality doesn’t lie. This is real.
Final Thoughts
By all means, the above peel-apart is far from complete. I’m sure there are more viral videos we could assess, more statistics to double-check, more anomalies to ponder. The point isn’t to reach a final conclusion here—just to demonstrate the process. The level of detail that must go into investigating a theory before we let ourselves fully entertain it. And if that process seems exhausting, excessive, excruciatingly nit-picky, too time consuming—well, it’s the price of admission for calling ourselves “informed.” Anything less and we’re operating on faith. Which is okay, if that’s our goal. But we must call it what it is.
Now maybe you’re thinking, “Okay, the ‘COVID-19 deaths are getting padded’ theory didn’t really hold up. But what about G5 radiation causing virus symptoms? What about mandatory vaccine agendas getting pushed on the world? What about COVID-19 being a bioweapon? What about what about what about?”
To which I say, Yes! Great! What about them indeed! Put on your best-tailored thinking cap and go find out. Marinate in all the data you can find. Watch out for claims that seem sciencey but trace back to a 4chan post. Be mindful of the universal human tendency to filter out things we disagree with and embrace any evidence that we like. Dig in, first and foremost, with the goal of proving yourself wrong. If you can’t, then perhaps there’s something there.
Of course, I realize the type of deep-dive we did in this post isn’t always possible, and not everyone can sit at home all day opening so many browser tabs that their MacBook freezes with a “System Has Run Run Out of Application Memory” error (anyone else? No? Just me?). Sometimes we need shortcuts. So for anyone who really wants to do the work, to prioritize truth-seeking over ideology, to stay oriented in reality, to let go of false narratives, but who doesn’t have infinite time to do so: here are some questions to ask whenever a new or alternative theory presents itself. Especially a theory we find ourselves enamored with. None of these questions can substitute for ruthlessly investigating, but they can help us stay grounded in situations where our minds easily lead us astray.
- Am I claiming to see through the media’s fear-mongering, but falling prey to conspiracy fear-mongering instead?
- Am I being pressured to accept this theory in order to be “woke” or “not sheeple”?
- Have I read the full context of this quote, clip, or screenshot before assuming I know what it means?
- Does the group promoting this theory invite questions and critiques? Or does it flippantly dismiss those things and/or attack its doubters?
- If this same form of evidence (Youtube interview, social media comment, etc.) was used to support the “other side” instead of mine, would I still consider it trustworthy?
- Am I taking time to research counter-arguments to these ideas, even when I want them to be true?
- Am I looking for good vs. evil narratives as a distraction from my immediate reality? Is getting worked up about hypothetical injustice easier than being present with what is?
- Am I embracing this theory as a way to feel like I have control—by naming an enemy in a situation where I’m otherwise helpless?
- Does seeing myself as a “good guy” on the side of “truth” or “justice” make me feel validated, empowered, and important?
It’s easy to trick ourselves into thinking we’re being Good Skeptics when we’ve really only lifted one veil of many. There’s nothing “woke” about rejecting the official story while gullibly swallowing its alternatives.
Rather, waking up means waking up to ourselves. It’s recognizing that the battle of good and evil we project onto the world is playing out daily within ourselves. It’s committing to seeing “what is,” instead of stories about “what is.” It’s spreading our skepticism evenly across the info-scape instead of saving it for the things we already distrust.
So here it is, you guys. This is me groveling at the collective feet of the internet, with one thing to say: to anyone—everyone—listening, we need to reflect on how we’re processing the claims we hear. If we’re going to question official narratives, we need to question alternative narratives with the same degree of rigor. There’s no use retiring our sheeplehood from the mainstream only to rejoin the herd on a different pasture.

Post-scripts:
- I now have a Facebook page where I post things sporadically and an Instagram page where I plan on eventually posting things sporadically. You’re welcome to join me over yonder!
- Hat tip to Kevin Bass for threatening to kill papayas if I don’t post this. It worked.

Holy Coronaspiracy, Batman! Denise is back posting! 😄
There really needs to be a “LIKE” button for this one!
Miss you
Thanks, Denise. Great to hear from you. “Proving yourself wrong” is the essence of science, and what real scientists do, or at least used to do, proof meaning something entirely different than the way we normally use it. Proof in science means to test, to design the test most likely to disprove one’s hypothesis. Thanks for helping us keep our eye on the ball!
People who don’t try to prove themselves wrong are not scientists. People who study the world with a prove myself wrong are scientists, regardless of degrees. Most of us switch between these states, depending on the subject.
IOW, credentials don’t anyone a scientist, nor does lack of credentials make one a non scientist.
That was an amazingly crafted piece. Well presented and enjoyable to read. I feel like it spoke directly to my brother who has been beating me over the head with his wokeness. I am hopeful your presentation, which I shared, will round out his thinking on these issues. Appreciate the mountain of work that must have gone into the post. Todd
>
Wow Denise!! We’ve missed you! This piece is amazing!
Wow Denise!! We’ve missed you! This piece is amazing!
Spot on.
Dr Dave Carsten
Sent from my iPhone
>
Yayyyyy you’re back!!!
Sent from my iPhone
>
Denise, great to see you back; sympathize with your despair over finding the truth behind food wars (“The Carnivore Code” has certainly thrown a spanner into my thinking), but be careful on this 5G and Covid-19 issue–there are at least two quite different u=issues mixed here; the first is whether EMF generally and 5G specifically may alter the virus to become more infective or whatever (I have no idea, but won’t rule it out totally at this point) and the second strikes me as very likely–this stuff can damage the human immune system, and render it less able to fight off pathogens. This strikes me as very likely indeed. So over to you on this one. Chris
S
I think we are all glad to see that Denise is back. Hate to hear her have mixed feelings about nutrition as a first line of defense, but that is another story altogether. Chris, I think the 5G is up for much debate, unfortunately, we probably wont have enough until it is too late in some cases. With the origin of this virus, and the possibility of it being man made or altered, nothing would surprise me. The older I get the more distrustful I have become of our government and many of the bureaucrats that work in it. Too many opportunities for data manipulation. Hopefully Denise will stay active, and apply her skills to get to the truth, even though it may not be palatable.
Jim
> The CDC has literally issued guidelines telling doctors and medical examiners to classify deaths as COVID-19 if they “presume” the patient has it—no test results needed.
It should also be pointed out that dead folks are not being tested for the simple reason that we don’t have enough tests for the live people.
> CDC mortality figures are initially very incomplete, low-balled-as-all-get-out, and retroactively fill in over time. Which means a weird pneumonia death-drop will show up any time we check the most recent data, COVID or No-vid.
So why are we not seeing the same pattern with covid-19 deaths? I suspect the answer is that we are putting out a tremendous effort to keep that data as current as possible because it’s needed to make informed decisions on dealing with this crisis, but that’s just a guess.
Hi Ed,
I think you’re right — they’re prioritizing reporting COVID-19 deaths for the sake of keeping the data as up to date as possible. Even so, there are definitely some lags there too with back-reporting deaths that happened at home, etc.
Thank you Denise for this wonderful post. Although I consider myself pretty rational, I had definitely fallen into exactly the trap you’re talking about. I appreciate you bringing me back to my senses.
I got email notification of your article on the controversy of the COVID-19 threat, and I appreciate your hard work, Denise. Am I to understand that you find statistics of actual total deaths per time period increasing around the time of the epidemic? In other words, actual body count would be a proxy or indicator for infection rate, and could not be faked. I’m researching this. While I’ve always seen this as a “real thing,” I did think it was exaggerated, but I could be wrong. I’m still not paranoid, but am concerned and not blind to the fragile nature of very life itself.
Denise! Thanks for this and glad to see you back again! xo
I eagerly started reading, but quickly realized, this ain’t suitable, for a 5 minute coffee break😄. Will come back later…but glad to see, you’re still alive and all!
Wouldn’t mind an update about your current view on nutrition, either…*hint*.
Spot on Denise. Nobody digs like you, Garry.
Great piece, Denise! Not that I would expect anything less from you. Please write more stuff. On anything and everything.
Great post, shame about the circumstances!
With regards to claim #4, I think the more rational among us are not worried that there is no extra mortality. Far more people are dying right now than usual, the evidence is clear.
The question is however, might the vast majority of people who died of covid19 died within the next 12 months? These graphs are terrifying, and very sad irrespective of who’s dying, but I do feel more useful data would be how many QALYs are being lost to covid, rather than “lives”.
There is a very high cost, economically and emotionally to the lockdown. We need to try to do accurate cost benefit analysis.
If your child were sick, you would give up your house and income in a second to save them and give them a full life. Most people wouldn’t do the same to give an elderly sick relative an extra 3 months in the nursing home, nor would I expect that they’d want you to.
It sounds horribly calculating, but in normal day to day life, medical interventions are assessed for cost effectiveness, why not now?
Perfect. This has been my principal point from day 1, plus the silly notion that you can contain the uncontainable—why we don’t do much to “contain” the annual flu that, even with a [typically shitty] vaccine, kills 300-600k globally each and every damn year.
Flu viruses mutate fast enough that we need a new vaccine every year. But the thing is — according to a radio broadcast I heard recently (sorry, Denise!) — that the take-up of the vaccine is very low. What should happen is that the whole population should get revaccinated every time a new vaccine comes out. What does happen is that even in the groups most at risk, few people bother. So, yes, it does kill hundreds of thousands every year.
Are you even aware of the ingredients in these vaccines? It turnes out one of the flu vaccines is now correlated with false positives for this insane pcr cerveza test. If you want to get these vaccines then I fully support your decision to do that. Count me out.
citations please
https://www.ncbi.nlm.nih.gov/pubmed/?term=influenza+vaccination+and+respiratory+virus+interference+among+department+of+defense
Robert T: The CDC now conflates influenza and pneumonia deaths into a single figure. While the”old mans friend,” pneumonia, does kill many each year, more than 100,00, influenza kills on average about 1,300 per year. In other words, influenza is not a major killer in the U.S.
It’s well known and established that you don’t die of influenza, you die of the pneumonia that ensues after the flu wipes out mucosal membranes, leaving it open for a bacterial infection…which is why early antibiotics are called for in serious flu cases.
2.5-4 million die of pneumonia every year, 2 million of them children under 5. Chief killer of them.
But the whole world is panicked over gramma and grandpa.
https://www.who.int/maternal_child_adolescent/documents/9280640489/en/
Well maybe we could if none of us ever leave the house again… 🙄
Hi Simon,
Thanks! It’s a very good question, one I’ve wondered as well, and I think the litmus test will be looking at what happens to mortality trends during the year or two after COVID-19 deaths drop back down to negligible. If mortality from chronic diseases stays depressed, and especially if there’s a reduction in expected mortality for the elderly bracket, that might be an indicator that this virus mostly wiped out people who didn’t have much time left anyway. If mortality returns to normal then it would be much harder to make that argument. (The one caveat being that we might also see changes in death trends related to whatever state the economy is in after this — e.g., sadly, suicides, and maybe increased death from normally treatable diseases among people who got hit hard financially and can’t pay for healthcare.)
I’m biased in my outlook on this because most of the people I know so far who died from this (at one degree separation — mostly relatives of friends) were in decent health and didn’t have pre-existing conditions. So that skews my own outlook. I’m hoping the future numbers contradict my personal experience.
As for #4, you’d be surprised how many rational people are still claiming there’s no excess mortality. The way information is flowing right now makes it hard to get a sense of the current numbers, since a mere month ago nothing looked alarming to anyone except infectious disease specialists, and many of us (myself included at the time) could only imagine linear changes from there. Exponential growth is a really hard concept for the human mind to grasp.
Thanks for your thoughts!
“…I think the litmus test will be looking at what happens to mortality trends during the year or two after COVID-19 deaths drop back down to negligible.” Denise, there is no specific test for Covid-19, so how in the world do you figure deaths from Covid-19 will be ascertained for those mortality trends?
Precisely. That one fact makes any speculation and evaluation of numbers (which is one of Ms. Minger’s fortes and the reason I’ve followed her so long and bought her book) completely erroneous. The very nature of the pcr test makes false positives a certainty.
As an aside, I ask everyone I speak with if they know anybody who has even been diagnosed with it…still zero. I live in an area with population around one million and every hospital I have visited is basically idle.
I live in CT. We have a father (in my town) younger than me and with kids about my kids’ ages in the ICU. In my county, as of yesterday (4/20/20), we have 8320 cases and 512 deaths. CT has has 19815 confirmed cases and 1331 deaths. 1919 are hospitalized from covid-19, mainly concentrated in certain locations. I looked at deaths from influenza in CT for the last decade or so, and that number is higher (by about 200 deaths or so) than the highest value I found, and that’s in two months, whereas influenza is for the entire year.
My wife’s niece works in upstate NY. She and her boss were using her boss’s house to work from to try to protect the boss’s mother who also lives in that house. The boss was just diagnosed with covid-19. The niece may or may not be able to get a test (the boss was symptomatic and that’s how he got a test, but she is not – yet). It’s unclear about the mother, as she fell and had to go to the hospital.
Are there wide disparities over the US? Absolutely. But if you look at just your location and say “nothing is happening”, be careful with that. Many other locations are overwhelmed. You may or may not be next.
I made no such implications but regardless of all that, the pcr tests being used to support your claims are highly flawed. The unscientific method the govt has mandated of just rubber stamping cerveza using visual cues (symptoms common to other conditions) only is self serving and further skews any data. No real protocols have been implemented to verify any of it. We should be able to harvest this virus from the blood of those infected but for whatever reason we cannot with this mystery bug.
If nothing else this debacle should reopen the debate between germ theory (yes the whole premise we are discussing is a theory) vs terrain theory. Allowing the govt to shackle us without a lick of the scientific method is an abomination. Environmental factors must be ruled out before we go issuing blanket directives. Damned sheep.
There is no test required. The point is to see if there’s a significant increase in overall mortality or not.
I.e. it’s estimated there’d have been around 60 million deaths globally in 2020 had Covid19 not happened.
If looking back at the end of the year there’s a huge spike in deaths in the first quarter, but then significantly fewer deaths than anticipated over the next three quarters, and the overall total is the same we’ll know that Covid was (probably) mainly just taking out people on the brink of death a little earlier.
If on the other hand there’s a huge spike in Q1, but the numbers are still as predicted in Qs 3-4 and overall mortality rate is much higher than the pre Covdi estimates, we’ll know that Covid (probably) had a big impact.
While it’s true that we’ll have a better idea after a couple of years (though of course we’ll never have the counterfactual), unfortunately we need to make decisions now.
The data from Italy is showing a mean/median age of 80, and 97% having a pre-existing medical condition.
If there were zero negative cost to social distancing, obviously it would be fine to wait for two years to see for sure if it was a good idea retrospectively or not, but sadly this isn’t the case.
I think at the very least we need to start having a serious conversation about the trade offs, and being realistic that we make cost-benefit analyses all the time that result in “lost lives”.
I.e. we could save many lives every year by banning cars, but no one is campaigning for that.
For what it’s worth, I choose not to have a car because I think the negative impact outweighs the benefits, but I’d look to at the very least greatly relax the restrictions ASAP as they simply don’t seem to be rational.
I cannot believe anyone ever started using the totally irrelevant and specious comparison of auto-related deaths to infection-related deaths, much less than anyone continues to waste time by repeating it. Let’s keep at least some bare semblance of logic in these discussions. Auto accidents are not contagious; they do not suddenly appear and increase at an exponential rate; each driver who is involved in an accident does not cause 2-3 other drivers to have an accident two weeks hence; we have the equivalent of treatment and vaccines for auto accidents — they are invariably due to human error. One could write several pages on the silliness of the “comparison”, but let’s not waste time doing that.
It is neither irrelevant nor specious.
The fact is that many of our everyday actions endanger the lives of others.
If you choose to get in a car and drive it, you risk running someone over and killing them, this is a fact.
The risk is low, but it is far from zero.
Currently, if you’re young and healthy, you have close to zero personal risk from covid, but you may inadvertently spread the virus to a more vulnerable person who then dies from the infection.
In both cases, your actions endanger the lives of others.
Also it would seem the treatment many have been receiving is proving incorrect – e.g. over use of ventilators. This is killing patients who may otherwise survive with correct treatment. It really is worth looking also at other countries who have a far lower mortality rate – e.g. S. Korea, Vietnam. Why is that? What are they doing that is different? Or are the people generally healthier?
Samantha Meyers: Also look at Bali. They should be dropping like flies, but they’re not. Likely they’re healthier, and no doubt strong social ties play a crucial role.
There definitly appears to be a correlation between rates of hospitalisation and ventilator use and increased death rates.
If this correlation us causal, I don’t think it’s likely that the ventilators are directly causing deaths, my best guess would be that it is bringing all the covid infected patients to the hospital to die increases viral load for medical staff and other patients.
It would seem better to give very sick patients palliative care at home.
The problem of course is that ventilation does appear to save some patients, between 10-25% depending on the study you look at.
Is it possible to more accurately identify these patients in advance and allocate these resources more effectively?
There is one thing few seem to be talking about. The reason we’ve been trying to control infections was not to necessarily to stop them entirely, although a vaccine might accomplish that end. More realistically, in the short term, there were two primary concerns. First, we wanted to avoid hospitals being overwhelmed. And, second, we wanted to delay most infections until better treatments were available.
Right now, because of lack of good treatments, not only are people dying who wouldn’t otherwise die but people are suffering permanent damage that will haunt them and the healthcare system for decades to come. Even if we don’t get the millions dead as with the 1918 flu, what if we get millions of survivors with severe health conditions and disabilities for life?
So far, there is no evidence that immunity results from recovery and we have no particular reason to assume a vaccine will ever be developed. SARS-CoV-2 could be more like tuberculosis in that once it’s in your system you’re permanently infected. There could be large waves upon waves of sickness and death over decades, if we don’t delay as many infections as possible.
It’s something to consider, as we don’t seem to know what kind of virus we are dealing with. The long term costs of the disease might be greater than the short term costs of keeping the economy shut down. But this requires we are capable of thinking in the long term, in delaying the short term gratification of getting things back to ‘normal’. Then again, if were capable of long term planning, we wouldn’t have been so unprepared for a pandemic in the first place.
I’m sure we will open the economy soon. It won’t be a rational decision based on good information. It will be simply driven by an anxiety to reinstate the dominant narrative of capitalist realism. Leave people out of work too long and they might start thinking too much about the corruption and injustice that created the weaknesses and failures in the system that allowed the pandemic to take hold at all.
The evidence so far indicates that the disease doesn’t pose significant risk to healthy individuals.
Lots of people have died, but 99% were very sick and likely would have died very shortly regardless. Obviously, we can’t know exactly when as we don’t have the counter factual, but as median age of those that died in Italy was 80 (and sick), one can presume not very long.
Both staying shut down and opening up will result in deaths the question is which will result in the greatest loss of qualys long term.
Obviously immediately going back to “normal” would be insanity.
I personally would argue for never going back to “normal”.
Equally however, strict lockdown until the disease is eradicated is also not a feasible choice.
The debate is what to recommence and how soon.
I’m not an advocate of an extreme position on either end of this debate. But I do think it might be wise to be cautious and slow in opening businesses. It’s never been a debate about absolutes.
Even in the shut down, large segments of the economy have still gone on running. Everyone I personally know here in Iowa is still working: healthcare workers, farmers, bakers, grocery store workers, postal workers, bus drivers, research lab workers, parks crews, county naturalists, golf course workers, lawn care services, etc. Even most restaurants have remained open, if only doing take-out.
We haven’t been shut down that long. And I’m living in the epicenter of where COVID-19 began in Iowa. The governor is already re-opening some businesses in counties with low infection rates, but she says they will base their decisions of further re-openings as more and better info comes in.
I should comment that I live in Spain, which I believe has the strictest lockdown.
After 50 days, finally on Saturday we’re going to be allowed out for a walk!
I’m lucky as work from home in a sector that’s thriving, but have many friends who are suffering terribly economically and psychologically.
I’m totally with you that we shouldn’t just go back to normal. Just that we should try and be rational and that attempting to minimise the daily death toll at any cost now might have consequences later.
Spain had a strict lockdown because it had one of the highest rates of infections and mortality in the world. I can’t speak for other countries or the justification of what other governments have done. All I can refer to is what is going on in the United States, which has differed greatly state to state with some states barely having shut anything down.
Overall, the vast majority of the US economy is still running. Everyone I know is still working. No one in the United States has been forced to remain in their homes, forced to wear masks, etc. US state governments have been mostly lax in their response. Even when people protest, the government does nothing in response. But you’re in a different situation. Your criticisms of your own government may be perfectly valid.
I’m not against moving toward opening more of the economy. Still, I resist those who dismiss the risks and want everything to back to ‘normal’ as quickly as possible. The United States is filled with reactionaries who are far from rational and reasonable. Plus, there are corporate interests that would push hard to getting back to business as usual even if it meant a high death count of their own easily replaceable cheap labor.
So, we are responding to very different situations.
I keep wondering about the potential permanent damage from COVID-19. We have a little bit of data on it. The virus can attack multiple areas of the body: lungs, spleen, nervous system, brain, etc. Some of the breathing difficulties, for example, might not be related to the lungs but to damage to specific cells in the brain.
There might be millions of people who seem fine now and yet could show serious health problems over the coming years and decades. Improved treatments over the coming weeks or months might be able to prevent most of those who otherwise would be harmed.
It’s not a reason to necessarily not open certain businesses back up. I’d just argue that it’s reason to take great care in how we do it, such as maintaining a basic level of social distancing and requiring protective gear be used while in public until we know what this virus does.
The mortality rate might end up being the least of our worries. Or maybe everything will turn out to be fine. But maybe we shouldn’t assume the best case scenario based on a lack of knowledge.
I think keeping everyone locked down because there “might” be unknown long-term serious effects is taking the precautionary principal too far.
Is it possible? Yes, but very very unlikely.
Conversely we know with 100% certainty that a major economic depression will result in greatly increased mortality.
Every time you leave the house or do anything you put yourself and others at risk, even without the virus.
But would permanently quarantining everyone result in longer life expectancy, and even if it did would it be worth it?
Yea. 100% speculation on his part. His sources for all this? Low iq politicians, state funded “scientists” and the lap dog media. I love all these experts which have fallen from the sky (including many commenting on this forum) after virtually nobody had even heard of it before a few weeks ago.
What has gone unnoticed is the unprecedented power transfer occurring from society to the state; I suppose the 250 or so million people slaughtered by their governments over the last 100 years is not enough for the bovine herd.
Unprecedented power transfer? There has been no power transfer to the state. Perhaps people have become more aware of the power the state already had?
But it’s hardly that simple.
The UK government planned to try a softer lockdown, and were soon kowtowed into line – where’s the power there?
It’s authoritarian leaning governments such a Bolsonaro’s that are resisting the lockdown. Claiming that the lockdown is some kind of state power grab just doesn’t fit the reality.
The fact is that most governments feel compelled to implement a lockdown as they fear that if they don’t they’ll be branded callous profiteers that value the economy over human life.
Conspiracy theories just don’t fit, as none of the usual suspects stand to benefit.
No state wants an economic depression, nor do big business, nor the oil companies. Yes, coronavirus makes great clickbait and media consumption is up, but advertising is down so they’re not benefiting either.
As for “state funded scientists” – if anything this whole debacle only shows how massively underfunded science has become!
The very fact governments can shutdown economies at the drop of a hat represents a game changing power grab. Your multiple red herrings expose how oblivious you are to the life or death importance basic economic activity represents…there is no such thing as a non-essential business.
You also seem to have forgotten the one country which ignored the globalist demand to lockdown all together. Sweden has made it through this without any of the silly protocols and economic shutdown and have attained actual herd immunity as a result. Not this faux immunity promised by Gates and Fauci via their vaccine fantasies; if that’s what you call science then go ahead and get the jab. Let me know how that works out.
Dude, I actually agreed with your original post. I was mostly responding to the Steele fella. Don’t know why you got triggered there.
I got triggered because you’re talking inflammatory nonsense, which then makes it much harder for reasonable people to try and make a rational point.
I’ve not forgotten Sweden. I think they are probably doing the right thing, and that maybe other countries should emulate them, though:
A) It’s still too early to tell and B) Swedes are totally different creatures to most other human beings in terms of behaviour and reasonableness, so it would be hard to say that other countries would get the same results from the same policies.
“The very fact governments can shutdown economies at the drop of a hat represents a game changing power grab.”
No it doesn’t. They’ve always had this power, they just didn’t exercise it because they had no reason to.
I believe in personal freedom, but that doesn’t make me want to live in a country with a failed or weak state that has no control of its economy or people.
We’re in a very strange situation here where it’s not exactly clear who wants the lockdown.
You seriously think that if Trump made a real power grab and were crowned absolute supreme ruler today, he wouldn’t simply open up everything tomorrow?
The almost sad fact is that there’s no grand conspiracy – nobody is secretly in control and pulling strings in the background, everyone is equally clueless!
You contradict yourself almost sentence by sentence and I doubt you are even aware of it. The fact people cannot make rational points has nothing to do with me; it is not possible for irrational people to make rational points. In times of universal deceit, the truth becomes “inflammatory”. The term reasonable is one of those unicorn terms which inches us towards outright tyranny, as is the word compromise.
If you believe in liberty then you certainly aren’t proving it with your words; non-contradiction, either/or, A is A…learn it, live it, love it.
The state is antithetical to freedom bro. If the last 100 years tells us anything it is that.
I’ve not said anything to contradict myself, just you.
“The state is antithetical to freedom bro. If the last 100 years tells us anything it is that.”
Well, no, it clearly doesn’t.
The US and Europe have very strong states, and lots of personal freedom, more than any time in history.
Our freedoms are now generally only ever restricted if our actions in turn restrict the freedoms, or otherwise pose a threat to other citizens under the protection of the state.
One such example would be restrictions on smoking.
As a libertarian, I’d be vehemently against an outright smoking ban, as people should be free to choose what substances they put in their own bodies. No one should be forced to be healthy.
I am in favour, however, of the ban of smoking in public places, as I want the freedom to go to these places without breathing in carcinogens.
You think that you’re going to be freer in a country with a weak state?
Go live in Somalia, Libya or the DRC and see how that works out for you.
Of course, a strong state doesn’t guarantee freedom. I certainly wouldn’t want to live in China or Russia either. But saying “State Bad, No State Good” just shows a complete lack of understanding of the world and human nature.
Though as it appears you like to just decide your own meanings for words, that’s hardly surprising really is it!
Yep. Not even aware. If your idea of freedom is the EU (a full fledged communist state) and US (fascist state transposing into a communist state before our eyes) then whatever public education you were inculcated with was 100% successful. Otto von Bismarck’s dream of the perfect citizen slave as been accomplished.
Before ww1 one could travel from London to Moscow without being asked for their papers even once; even if you happened upon a local monarchical dust-up. Same with the US. That is what you call freedom. The serfs of Europe were more free than an EU citizen.
So your ideal world is that of pre world war i? That worked out well didn’t it!
The EU communist 🤣
Oh my word, you really do need to get a dictionary.
From a freedom perspective absolutely it was far better; it was actually the death Queen Victoria which set the stage for the death of liberty in Europe.
No counterfeit money masters and their usury, no corporate/communist state, self responsibility and autonomy instead of the nanny state. Your slave mind cannot even fathom a world where the consent of the governed rules the government.
I certainly do not need a dictionary, but you need a history lesson. The last century saw the socialist agenda being instituted first by force, then by public education; we are now stuck with mindless youth addicted to their monitors. You do not even provide real responses, just your millennial level emojis and empty bromides; how pathetic is that?
Well this does make a refreshing change to arguing with socialists bemoaning the rise of neoliberalism.
Your only “evidence” of increased freedom, was a claim that you could travel from London to Europe without a passport before WW1. While technically true, in practice this type of journey wasn’t feasible for 99% of the population as it would have been a very long and expensive journey.
While London to Moscow without a passport might not be possible, Lisboa to Talin is. Plus the journey can be done fast and cheap, and you can decide to stop, live and work anywhere along the way.
That’s just freedom of movement.
In your amazing free and democratic Victorian era, homosexuality was a crime, women couldn’t vote, abortion was illegal. But you’re probably a straight white male boomer so not too bothered about those freedoms.
I’m a straight white male too. But I’m gen x so I’m a but more woke than you, while still knowing a bit more history it seems 😘
You certainly have not displayed any knowledge of history in this conversation. The fact you would put democracy and freedom in the same sentence exposes your ignorance. History shows democracy precedes tyranny 100% of the time.
I did not imply it was perfect then, just better. Taxes and administration were much, much lower. Conflicts only included small fights in which only soldiers died, not the all out war where civilians were slaughtered. Again there were exceptions to that but nothing like now.
I think WW1 should be classed as a little more than a small fight
As I said, the death of Queen Victoria was the turning point but given the consequences of the French Revolution, I’m not sure even she could have kept WW1 from happening despite being the grandmother of the king, czar and kaiser.
The latest developments in Hungary are disappointing, I will grant you that. Orban surprised me.
I honestly have not noticed any logical argument from you. When I stated one did not have to show a passport, that is because there was no such thing as a passport. Free travel is a God given natural right, not a privilege granted by sniveling bureaucrats in Strasbourg.
It should also be noted that under normal circumstances I can travel from my house in Barcelona, all the way to the border with Russia without the need to show my passport. I’m also free to live and work in any of those countries.
Barcelona??? No doubt you supported the tyrannical crackdown of the Catalan Independence Movement; and you call yourself free. Have they even let the political prisoners out of the dungeons there yet? What a joke. What’s it like to live on your knees?
When I call the EU communist, I am mostly referring to southern Europe. Such a high concentration of beta males there. I have generally limited my visits to the EU to areas such as Czech Republic and Hungary where they at least pay lip service to freedom.
Discussing liberty with someone from Spain is the same as doing a card trick for a dog and expecting any response. Just a blank out.
Hungary? Wow, you really know how to show your ignorance don’t you.
You pick one of the two EU countries where there has been an actual power grab and is no longer a free democracy 🤓
By the EU most people refer to the EU. Again, you’re failure to use words makes having a sensible conversation tricky. I presume when you say dog, you mean cat?
Even if you mean Spain and Italy however, neither are communist. Barcelona was briefly, but then they lost the civil war. Both countries spent most of the last century under the rule of fascist dictatorships.
They haven’t released the political prisoners yet FYI. I never said I lived in a utopia. Obviously there’s things I’d change. I’m not in agreement with how either side handled that debacle, and I’m not in agreement with the lockdown either. I’m not in agreement with many of the policies over here. Taxes are too high, over regulation, etc.
I’m not Spanish though, I’m English. I live here out of choice, as while it’s not perfect, it’s my preferred free choice.
I note that you haven’t responded to any of my actual points, other than ad hominem attacks. Wonder why that might be… Oh because you’ve no idea what you’re taking about.
First off, in the US, we aren’t in a lockdown, much less a takeover by an authoritarian police state. There are restrictions. But most of the economy is still running. Most Americans are still working. And Americans are still free to go outside, travel on roads to go places, etc. For the average person, there is very little enforcement going on.
Many states have open a wide variety of businesses far beyond grocery stores: big box stores, gardening stores, etc; even restaurants, theaters, beauty salons, and much else. Beaches have also been opening again. Here in Iowa, people are out enjoying the parks, although the bathrooms are shut down.
The mild response from state governments in the US doesn’t seem unreasonable. It did achieve one of the main intended purposes, the slowing down of the infection spread so hospitals wouldn’t be overwhelmed. This has also given us some breathing room during the research and development phase involving immunity, vaccines, and medical treatments. We’ll probably be seeing major findings in the coming weeks that could save large numbers of lives and prevent much harm.
I haven’t heard of anyone in the US calling for a total lockdown with no end in sight. The places in the US that had the greatest restrictions were in response to having the greatest rates of infection and mortality, a perfectly rational and moral response to the situation, especially given the limited knowledge at the time. Waiting a short while longer to get our bearings before jumping back into ‘normalcy’ doesn’t seem wise. But that isn’t to say we shouldn’t be moving in that direction.
It’s not about preventing all risk but about preventing the greatest risks. We can disagree and debate about that. But creating a caricature of one’s opponents is not helpful. No one is fantasizing about the elimination of all potential deaths and harm. Depending on how we move forward, we could be talking about hundreds of thousands or even millions of people in some countries who are saved from permanent health problems. Isn’t that worth waiting a few more weeks to see what we learn?
That said, the US theoretically is a democracy, not that it functions that way most of the time. The federal government has little power to tell state governments what to do. If the majority of residents in particular states demand that the economy be re-opened, then more power to them. As an experiment, I’d actually support a full ending of all restrictions in some state and see what happens, assuming that is what the local citizenry wanted. But so far, most Americans in most states are still in support of maintaining many of the restrictions for the time being.
By the way, I agree with your assessment of Sweden. Americans are not the Swedish, not even slightly. The Swedish have a high tax rate, a functioning social democracy, a well funded welfare state, strongly organized labor unions, and universal healthcare. They also have a culture of trust where the government is more trusted, as opposed to the paranoid conspiracy theorizing that dominates a reactionary society like the United States. Also, compared to the rest of the world, they have the highest rate of single people living alone. Unlike the US, they were prepared for a crisis like this.
Still, as suggested, I’d love to see some liberty-loving state in the US, maybe South Carolina or Alabama, try to go the Sweden route or what they imagine it to be. The reality, though, is that even Sweden implemented many restrictions over time. Sweden didn’t do a full lockdown, but then again neither did the US. So, the fantasy about Sweden is a bit blown out of proportion. Besides, it is true that Sweden had a higher infection and mortality rate than its neighboring countries that implemented more restrictions. All of that should be part of a reasonable public debate, if such a thing were possible in the United States.
It will certainly be interesting 2-5 years down the line to see what effects different approaches have had on both total mortality and the economy.
Of course, one can never know for sure as A) there’s so much heterogeneity between different regions applying the same tactics already B) as previously noted, even if an approach was “the right one” for one place, doesn’t mean it would have been for another.
That is the thing for me. I’m all for democracy and I’m all for experimentation. That is one of the advantages of a federal system like the United States. Almost all the power for public health is at the local level, even though most of the funding for public health is at the federal level. States in the US have not been the same in their responses.
I wish different places took entirely different approaches, simply for the sake of being able to do later comparisons. But you’d need places with similar populations, cultures, economics, climate, etc. So, maybe Sweden compared to Finland or, in the US, maybe Texas compared to California. Even then, comparisons would be imperfect since the confounders aren’t controlled.
Anyways, similar to US federalism, Italy is another good place to look for comparisons. In Italy, the response to COVID-19 was local, specifically by province. The Province of Bergamo was hit the hardest and they had a weak initial response, whereas a neighboring province also in the north had a strong response with a much smaller infection and mortality rate. Was it the response that made such an impressive difference or other factors?
When looking at the worst hit places in Italy, Spain and the US, they share some common features. In particular, high levels of poverty and inequality. As or Italy and Spain, they had the additional problem of austerity economics that put them in a bad situation for health crisis preparation.
I’m not sure you can really blame poverty. If anything, I’d say a major reason that we’re seeing such high death rates across Europe and US is because these countries are wealthy.
Most deaths occur in octogenarians with multiple pre-existing health conditions. In poorer countries these individuals would have died long ago of something else.
Not that I’m saying that poverty and inequality aren’t problems within these nations. They certainly need addressing.
I will grant you of course that if you compare within a country, the poorest almost always suffer more and die younger, but if we compare across time or globally even the poorest in these nations are living longer than any other humans anywhere, any time.
It’s the age old juggling act between growing the pie and sharing the pie…
https://www.livenowthrivelater.co.uk/2020/04/lockdowns-longevity-liberty-long-termism/
We could disagree about analysis and interpretation. But the data across numerous countries shows that one of the greatest comorbidities is poverty. That is to say that many of the comorbidities affect the poor more than the rich, since their inequalities in access to healthy food, healthcare, green spaces, etc.
I’d make a couple points about people living longer in these high inequality societies. We have to be careful because national longevity rates are averages, not indicating the inequality in longevity within a given society. Also, longevity rates among the US poor are now declining, but not seen among the wealthy.
To offer a larger perspective, longevity of some more primitive societies is only shorter because of infectious diseases in childhood (by the way, some of those infectious diseases originated in agricultural societies that are breeding grounds for new diseases). But their average lifespan is about the same as ours, once beyond childhood.
Not only that but hunter-gatherers have few of the chronic diseases that are the comorbidities we are seeing. They live about as long as we do while their healthspan is much longer. Hunter-gatherers and others in many traditional societies tend to remain healthy into old age, working and helping out their families until they die.
That said, it’s true that human longevity drastically fell with the agricultural revolution. That is seen in height and brain size. We are only now regaining the height of Paleolithic humans, but we have yet to regain their brain size. Comparing poor agricultural societies to wealthy agricultural societies might not be as useful, since it vast inequality never existed prior to agriculture.
Modern inequality is not only within countries but across them. All of our economies are interconnected with a colonial and post-colonial history of exploitation and environmental devastation. We in the wealthier countries have gained many of our advantages from externalizing costs onto poor countries. But the disparities even within some countries can be stark. Parts of the US in te Deep South have poverty and health outcomes as bad or worse than many developing countries.
“But their average lifespan is about the same as ours, once beyond childhood.”
This is basically like saying, they’d live as long as us if they didn’t die earlier…
Yes, if you discount all the horrible things children die of in primitive societies, they’d live nearly as long as us. Great!
But then you’d have to discount all the lovely things we die of in modern society – not enough arduous physical work, delicious high calorie easily available food, motorised transportation, etc.
I am not trying to suggest that poverty isn’t a bad thing that we shouldn’t worry about.
Inequality is more complicated however.
Is it better to live in an unequal world, with wealthy people and incredibly wealthy people, or an equal world where everyone is poor?
Of course, it’s an impossible question because wealth and poverty are relative terms.
I would agree though that it would be nice to live in a world with “health equality”. Maybe this is possible one day, if there’s some kind of limiting factor to longevity?
Some thoughts on this –
Imagine a world where everyone died at 60 rich or poor, this would be equality, it would be normal and everyone would be fine about it.
But if one day wealth could pay to extend a life to 80, there’d be an inequality, which seems unfair on those that still die at 60. Is it a worse world?
If they reached 80 by stealing years from the others who now died at 50, that would certainly seem bad.
But what if actually in the process they extended the others lives to 65. Now you have a world where everyone is living longer – still unequal, but surely better?
Then the next generation live to 75 and 85, and so on.
This is basically the world we live in.
Will we eventually reach a biological ceiling where money can’t buy you more health that will allow the poor to catch up? Or can we keep pushing the limits forever? Will we end up with immortal billionaire cyborgs with an underclass of mortal meatbags? Would we have been better off just staying the forests as hunter-gatherers blissfully ignorant?
You write that, “This is basically like saying, they’d live as long as us if they didn’t die earlier…” I get what you’re saying and I’ve heard this counter-argument many times before. But I’d argue that it’s not the same. Or rather it misses the point I’m trying to make, albeit maybe I’ve failed to communicate it well. I’m not romanticizing ‘primitives’, but it’s helpful to recognize what the differences mean. Hunter-gatherers lack the medical care to deal with infectious diseases and traumatic accidents. Then again, many of the infectious diseases of hunter-gatherers come from contact with those who aren’t hunter-gatherers, often originating in agricultural centers and crowded urban areas.
No one is arguing that antibiotics aren’t a good thing, specifically in modern society where infectious diseases proliferate so easily, nor other medical advancements. A main issue is that, if hunter-gatherers had ready access to antibiotics (and emergency care for accidents), their greater health in adulthood would translate into greater longevity to match their greater healthspan. That is to say, if we had their diet and lifestyle, our own health would be improved. It’s important to understand the difference between longevity and lifespan and between lifespan and healthspan. Without that understanding, it is impossible to explain the meaningful differences. Hunter-gatherers have low rates of chronic diseases, from metabolic syndrome to autoimmune disorders. That is why they have the same lifespan as us and even longer healthspan, even though their longevity is shorter.
This difference is not an insignificant detail, specifically as it is chronic diseases that are comorbidities in adult infections. Despite having more childhood infections, hunter-gatherers have lower rates of infections in adulthood. Living a traditional lifestyle and eating a traditional diet, hunter-gatherers would unlikely be much affected by COVID-19. To put it in context, I highly recommend the work of Weston A. Price, as the photographs he took comparing populations are powerful in how they show the immense variations in health, largely dependent on diet and nutrition. The contrast is stark. But what really stands out is how few people in the modern world look close to as healthy as those from the healthiest societies of the past.
I live in a fairly wealthy college and medical town where there is a far above average concern for health along with access to healthcare. Even so, I now can’t help noticing how many people around me show signs of stunted or perturbed development of the exact kind Price observed in great detail: thin bone structure, sunken chests, sloping shoulders, narrow facial features, asymmetry, etc. That is even with modern healthcare correcting some of the worst conditions: cavities, underbites, pigeon-toes, etc. That is on top of the 88% of the US population suffering from metabolic diseases (obesity, diabetes, heart disease, etc). My fellow residents in this town are among the most privileged people in the world and, nonetheless, their state of health is a sad state of affairs in what it says about humanity at present.
That brings me to my next point, in response to a question you asked: “Is it better to live in an unequal world, with wealthy people and incredibly wealthy people, or an equal world where everyone is poor?” Inequality is not only about wealth but, more importantly, about disparities of resources, opportunities, infrastructure, class privilege, social influence, political representation, etc. It’s true that the people who die are those with comorbidities. But stop for a moment and consider who are these people. It’s specifically the poor who have the highest rate of chronic diseases. Why? It is caused by inadequate or unavailable healthcare, polluted air, water, soil and housing (from heavy traffic areas, toxic dumps, aging infrastructure, old paint, and factories that used to be located in inner cities), food deserts, stress and trauma (particularly Adverse Childhood Experiences), lack of green spaces and safe places to play/exercise, and on and on.
Poverty in a low inequality society like that of hunter-gatherers is extremely different than poverty in a high inequality society of modern industry. Even in Western developed countries, the differences can be stark. In high inequality US, people have worse health and shorter lives than those in most other Western countries, even those far less wealthy. Even the upper classes are worse off in a high inequality society, as the data shows. Much of it has to do with the conflicts and stress that are inevitable under vastly unequal conditions. To fully appreciate this, I’d recommend reading Keith Payne’s The Broken Ladder along with the work of Kate Pickett and Richard Wilkinson’s, specifically The Inner Level. Payne does a really good job of explaining why wealth is such a small part of inequality.
Others point out that democracy is impossible in a high inequality society, as democracy necessitates a basic level of egalitarianism. As inequality grows as it has in the US, socioeconomic mobility decreases and corruption takes hold. In the past, it was understood that a defining feature of banana republics is high inequality. It creates the conditions for conflict and division, fearmongering and scapegoating, political polarization and authoritarianism. It’s the rich loam of the reactionary mind that takes hold like a weed across the political spectrum and the economic classes. From Payne’s book, here are two good parts where he discusses the research, one about polarization and the other about how high inequality mimics poverty — here is the first (pp. 110-111):
“Political scientist Nolan McCarty and his colleagues have also traced political divisions over the last century in the U.S. House of Representatives and Senate, formulating a measure of polarization based on how lawmakers vote, similar to the data used for Andris’s graphs. The polarization index is at its highest when all Democrats vote one way and all Republicans vote the other. Using this index, they calculated how polarized American politics has been in every Congress since 1947. Figure 4.5 shows that polarization in the House of Representatives and the Gini index of inequality have followed strikingly similar trajectories. Results for the Senate are similar. Both inequality and polarization were relatively low through the 1950s and 1960s. They then began rising in tandem in the mid-1970s and have remained on par ever since.”
And (p. 3):
“But they do not act strange in just any old way. Inequality affects our actions and our feelings in the same systematic, predictable fashion again and again. It makes us shortsighted and prone to risky behavior, willing to sacrifice a secure future for immediate gratification. It makes us more inclined to make self-defeating decisions. It makes us believe weird things, superstitiously clinging to the world as we want it to be rather than as it is. Inequality divides us, cleaving us into camps not only of income but also of ideology and race, eroding our trust in one another. It generates stress and makes us all less healthy and less happy.
“Picture a neighborhood full of people like the ones I’ve described above: shortsighted, irresponsible people making bad choices; mistrustful people segregated by race and by ideology; superstitious people who won’t listen to reason; people who turn to self-destructive habits as they cope with the stress and anxieties of their daily lives. These are the classic tropes of poverty and could serve as a stereotypical description of the population of any poor inner-city neighborhood or depressed rural trailer park. But as we will see in the chapters ahead, inequality can produce these tendencies even among the middle class and wealthy individuals.”
As I’ve made clear, I’m skeptical toward those who would deny the seriousness of this COVID-19 pandemic. But I don’t dismiss all of the critics out of hand. Some are correct about certain issues. Many (most?) pandemics are to varying degrees socially constructed, in that if the conditions were changed they likely wouldn’t happen or not as badly. The 1918 flu was a perfect storm of concentrated populations, industrialized diet, international conflict, disrupted trade, refugee crises, large troop movements, etc; not to mention all the problems related the worsening inequality with big cities, industrial capitalism, and proto-neoliberalism. By the way, the early 1900s was when Weston A. Price was practicing as a dentist and when he began to travel the world in studying population health. In many ways, we are further down the same path of public health crisis that has been developing for generations now.
The straightforward elements of health are key, of course. Americans and many other modern populations have higher rates of chronic diseases than ever before in history. And though longevity on average has decreased, it has not done so evenly. The longest lived tend to be the wealthiest, whereas in the US the lower classes have begun to have dropping longevity. The societies with greater longevity than the US aren’t wealthier but they do have lower inequality. The inequity doesn’t only affect personal health but also public health. Greater disparity between rich and poor erodes public trust and, as the upper classes gain increasing power, they are ever less willing to invest in the public good, including public health.
That is how we get someone like Donald Trump as president who left positions open for security officials handling pandemics and tried to defund the CDC, and he has continually attacked scientific experts since elected. The economic populism incited by high inequality was attacked by the DNC in their punching left which allowed right-wing reactionaries to take advantage of the widespread sense of injustice and corruption. This then left us even more vulnerable in lacking an organized public response when it was most needed.
I’m aware of the arguments made by the Weston Price Foundation and proponents of the Paleo diet.
I used to drink that cool aid too. Sadly it’s highly flawed for many reasons.
A significant one is that of survivorship bias. You can’t compare the average health, strength and intelligence of adult hunger gatherers with modern humans because only the healthiest, strongest and most intelligent survived.
A quick way to increase our modern averages would be to cull/let die all the weak, sick or mentally handicapped babies…
I wrote about these errors many years ago here: https://www.livenowthrivelater.co.uk/2012/05/diet-debate-the-problems-with-paleo-science-and-why-it-matters/
I spend months every year thru hiking in the mountains. I love the outdoors, handicrafts, self sufficiency, etc. But I am also very happy to have access to modern medical care and return to the comfort of my own home at the end of it all.
I fully agree that wealth is associated with increased health and longevity.
I agree we should aim to lift people out of poverty, but simply believe that we should think in absolute rather than relative terms.
There’s a huge wealth inequality between myself and Bill Gates, but so what?
I have everything that I could ever want or need. He’s currently using his vast extra wealth to try and help with this situation. Even if he wasn’t and was just spending it on frivolous things, he’d still be paying people’s wages and improving their lives.
Our aim should be to ensure that everyone has enough, not that everyone has the same.
Another thing to note is that you could quickly increase healthspan in the US by banning fast food and forcing people to do more physical activity.
Cuba has a longer life and healthspan than the US despite being vastly poorer.
Does this mean that Cuba is the better place to live?
You don’t actually have to be rich to be healthy. You can exercise for free, and eat a healthy diet for free (nb a major problem with Weston Price and Paleo is that they would make it seem that health eating is only for the wealthy, when in fact you can do so very cheaply).
If health and longevity were the only things that were important, fixing the issue would be easy.
But freedom and progress are also important factors, so it’s necessary to keep a balance.
If you say poverty kills, yes, it sounds terrible. But I don’t think the facts really show that.
More that wealth extends and improves all lives, and we should keep generating more until everyone has more than enough.
I’ve been trying to respond to you. But WordPress won’t post my comments. I assume they are being sent into Spam or Trash. I even tried eliminating all links from my comment and it still wouldn’t post. Hopefully, Minger will notice and retrieve my original comment with all of its links.
I’m sure Denise has better things to do than read all this ☺
It’s funny, talking with you and wondering scholar makes me think of the scene in Life of Brian “What have the Romans ever done for us”.
Obviously you both come from opposite ends of the spectrum (well, ok maybe our friend WS has wondered off the edge of the spectrum altogether), but you’re both only able to see the faults of the opposite side.
Yes, if hunter gatherers had vaccination, antibiotics and hospitals they’d be healthier than us.
And they do, we are hunter gatherers with vaccinations, antibiotics and hospitals.
But we also have McDonalds, Whole foods and Amazon. So most people don’t hunt and gather anymore either.
Can and should you have the former without the later?
Are people that choose soda and smoking over optimum healthspan wrong? Should they be coerced into “better decisions”?
I see many sides of the debate. I’m not a radical left-winger by any means. When I look at American public polls, my views tend to fall mostly somewhere in the middle. But admittedly so much of our political system has been pushed far right, which distorts what is perceived as the ‘middle’. So, in terms of politics and social views, the only opposite end I’m on is opposite of minority opinion.
I was raised by conservative parents, some combination of social conservatism and libertarian values. I also spent much of my youth in the Deep South. Beyond that, I’ve regularly explored alternative thinking across the spectrum from listening to right-wing talk radio and Art Bell in the 1990s to exploring HBD, ancap, etc online in more recent years.
My dietary views, however, do put me outside of the majority. Then again, my dietary views also don’t exactly line up with typical politics. I’m more on the political left, if not extremely, but those who share my dietary views are often on the libertarian right in being critical of government guidelines and such. Traditional foods, paleo diet, etc tend to attract many right-wingers for some reason, the same kind of people who home school their kids and collect guns.
I’m fairly liberal and am surrounded by liberals. Yet I regularly criticize liberals. My emphasis on animal foods puts me in opposition to most liberals who idealize vegetarianism and veganism or at least ascribe to the ideal of eating tons of plant foods.
Anyway, here is the basic point I made in my comment that wasn’t posted. The issues of inequality and health aren’t only about quantity of dollars and quantity of years but, more importantly, about quality of life and quality of healthspan. The average American may live a reasonably long life but they likely will do so with high levels of stress, horrible health, chronic diseases, neurodegenerative conditions, and mood disorders.
Those are all related to the reasons they have greater vulnerability to infectious diseases like SARS-CoV-2. That is the context of our discussion, after all.
Around 10 years ago when I was a paleo guru, I had much more traditional left wing views.
It’s an intresting question if there are correlations between political views and dietary beliefs.
Nb I was veggie / vegan for 13 years before that. Make of that what you will!
High levels of stress, horrible health, chronic disease, etc… These are not exclusive to modern Americans, this is simply the human condition.
If primitive societies had fewer of any of these things, it was simply because they quickly resulted in death.
Likewise with covid, as per my original point – the main victims are 80 year olds with multiple pre existing conditions who in any other era or society would already be dead.
Plenty of people still have shit lives, through pure bad luck of birth, this is true. But this has always been the case.
If reincarnation were a thing, you’d have a much better chance of a longer and less miserable existence in this modern era, than in any previous one.
Parasite load, specifically of hookworms, is an example of immense disparities between not only wealthy and poor countries but within wealthy countries like the United States. Keep in mind that parasite load has a major impact on general health, including neurocognitive development, but research shows it also affects culture, according to the parasite-stress theory.
So, investment in public health, as seen with Sweden, could be one of the factors for why they have a culture of trust. But it’s a virtuous cycle since increased culture of trust allows more funding of the public good. Countries like the United States, instead, are trapped in a vicious cycle spiraling down into ever worst outcomes as seen with growing inequality in both wealth and longevity.
That is what most o those praising Sweden ignore.
https://en.wikipedia.org/wiki/Parasite-stress_theory
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124128/
Can someone explain to me why everyone thinks there is no immunity from this infection? Has everyone’s immune system suddenly been turned off?
Is it because of the tweet that the WHO sent out then deleted because it was so wrong? (“There is currently no evidence that people who have recovered from #COVID19 and have antibodies are protected from a second infection.”)
People who think there is no immunity should have told the people conducting several clinical trials currently underway in which plasma from infected individuals chock full of antibodies are being injected into people infected with the virus.
UK approves clinical trial of plasma therapy for Covid-19, April 27, 2020
https://www.clinicaltrialsarena.com/news/uk-covid-19-plasma-therapy-trial
In fact, there is already evidence from March 27, 2020:
“In this uncontrolled case series of 5 critically ill patients with COVID-19 and acute respiratory distress syndrome (ARDS), administration of convalescent plasma containing neutralizing antibody was followed by an improvement in clinical status.”
Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma
https://jamanetwork.com/journals/jama/fullarticle/2763983
So the idea that there is “no evidence” is clearly wrong. It’s because of the evidence above that clinical trials are underway.
Moreover, Sweden is seeing a reduction in cases in part due to herd immunity being built up.
Here is just one of thousands of articles on the topic (“sweden builds herd immunity” –> About 891,000 results (0.67 seconds) )
Swedish official Anders Tegnell says ‘herd immunity’ in Sweden might be a few weeks away
https://www.usatoday.com/story/news/world/2020/04/28/coronavirus-covid-19-sweden-anders-tegnell-herd-immunity/3031536001
And logic 101 means that if antibodies from the natural infection won’t protect then how the heck is a vaccine that produces antibodies supposed to protect?
Seriously. People just aren’t thinking.
I think I know what’s happening: people are so afraid of contagion it’s impacting their cognitive ability.
I’m actually not kidding here. Our exquisite immune system is the result of the arms race between pathological organisms and humans (actually, much earlier). I bet if I look in the literature I will find evidence that certain behavior can be tied directly to the fear of infectious disease. I would start with morning sickness and go from there.
So people hear someone say, “there is no evidence,” the topic is contagion so their brain turns off (“get away from it immediately!”) and thus access to hundreds of years of knowledge about the immune system is no longer accessible.
How can one remain skeptical about what we don’t yet know for certain? It’s called the scientific process. There is conflicting data right now. Maybe to put it differently, let’s agree that the evidence is unclear. The gaps in our knowledge are immense.
We simply don’t know much about possible immunity to SARS-CoV-2. But we do have reasons to suspect immunity could be possible, although there is evidence that at least some people might get re-infected. Time will tell. Let’s wait for research to clarify the matter. It’s not going to be solved in the comments section of a blog.
Even if immunity turns out to be real, there are additional problems. It might be short-lived, only lasting weeks or months. But assuming it does last longer, the rate of infections now would mean we wouldn’t reach herd immunity until years from now. In that case, we better hope a vaccine is developed quickly.
https://www.medpagetoday.com/infectiousdisease/covid19/86171
https://www.scmp.com/news/china/science/article/3082069/researchers-report-more-people-covid-19-antibodies-and-its
https://www.factcheck.org/2020/04/qa-on-covid-19-antibody-tests/
https://www.independent.co.uk/life-style/health-and-families/coronavirus-immunity-reinfection-get-covid-19-twice-sick-spread-relapse-a9400691.html
https://www.technologyreview.com/2020/04/27/1000569/how-long-are-people-immune-to-covid-19/
https://www.philstockworld.com/2020/04/29/what-if-covid19-immunity-doesnt-last-long/
“It might be short-lived, only lasting weeks or months.”
That’s reasonable. To say there is “no evidence” is not reasonable especially with our knowledge of the antibody transfer studies now underway.
That is fair enough. I should have been more clear in what I meant. The main issue is that I wouldn’t bet on immunity.
Of course, there is all kinds of evidence. It’s not like scientists have never studied coronaviruses before. Then again, this isn’t like other coronaviruses.
There is a good chance that a certain degree of immunity will be likely, at least for some individuals for some length of time. But I guess, for now, I’d say the Devil will be in the details.
That is my concern. We don’t know the long term effects of COVID-19. I’d like to see more public debate about that, far beyond only issues of mortality and immunity.
Mystery solved: they weren’t reinfections.
Dead coronavirus fragments likely caused positive test results in recovered South Koreans, officials say
https://thehill.com/policy/healthcare/public-global-health/495488-dead-coronavirus-fragments-likely-caused-positive-test
The mystery isn’t solved. It’s just more info to be considered as possible evidence. Even the title points out that this conclusion is not absolutely certain, in referring to it as ‘likely’. So, sure, it’s important info to consider. It’s not like I’m hoping there won’t be any immunity. I’ll be as happy as can be, if and when they can prove immunity happens for all or most people and that it lasts for a long period of time.
I ask myself the same questions regarding society’s current cognitive dysfunction. Somewhere in the course of human events vaccination became conflated with herd immunity; Sweden obviously did not get that particular memo and they are better for it. I contend this example of contradictory identification did not just fall from the sky, which of course goes squarely against the very premise of this blog post.
Excellent point!
Great article Denise. Just one point the thinking 5G opponents are working from a theory that 5G may lower our immune systems ability to respond but the press seem to prefer to focus on the daft idea that 5G somehow causes the virus. The latter is crazy whilst the former is plausible and worth investigating as many independant Scientists are doing
Sigh! It used to be relatively easy, albeit occasionally time-consuming, for science-types to debunk the fantasies of crackpots that the “gubmint” is up to something sinister. Sadly, we now have crackpot “gubmint” officials spreading fantasies that “the scientists” — some of whom (gasp!) use MODELS! — are up to something sinister. Why, it wouldn’t be surprising if “the scientists” are part of that same cabal that’s been pushing the idea of human-generated global warming, motivated by their base desires for … something/something/something. Yeah! Those guys used models, too! 😉
Hi! thanks. I have my own view on how to reconcile “coronaconspiracy” views with what could have happened in the last few months. A hypothesis a la John Le Carre, how big players are trying to make the most of it (I see 4 actors in the play). Hope you can have it translated, it is a llllllong post in fb: https://www.facebook.com/taty.lauwers/posts/2883996661669831
Denise, I was only thinking a couple of days ago – we haven’t heard from Denise for eons, I wonder what she is up to and surely she would have something to enlighten us with and clarify the muddled thoughts in our heads as family members start reposting all the conspiracies (with clearly more time than is good on their hands) – many of them falling down into the terribly addictive rabbit hole of Youtube conspiracy theorists. Thank you – your blog is very timely. You are amazing. Can you do 5G next please and then I have a list of others after that…
Hope life is good with you and yours x
Well Denise, you also missed the broader context. In general this pandemic is clash between two worldviews. And both sides use data for their own good. Even those who proclaim they have no belief, operate through the belief. But this time belief of objectivity and numbers. Maybe instead of trying to prove which side is wrong, we have accept that there are different realities. That we have to learn how to operate in different realities. How to make decisions in such a society? Still with the power? It looks it does not bring anything at least long term. Maybe we have to accept that there are no one size fit all policies. Maybe we have to accept that any step makes mistakes possible? In homeopathy you have a term – miasm which basically means disposition to disease. So when you look at this disease and current state of world, it is no surprise we have it. But instead of looking at it from more inclusive angle we waste our time in throwing data at each other.
Talking about numbers, I just read discussion in The Netherlands that numbers what is given by Euro Momo do not conform with the numbers from CBS (dutch bureau for statistic) and they also do not conform with the number of RIVM (dutch CDC) (to be clear the numbers of CBS and RIVM are also different). They are still waiting for answer from CBS where this mismatch comes from.
Pleased to see a new post from you. And then disappointed to see not a single sentence touching on the concerns people have over whether state-wide lockdown is a proportionate and sensible measure, and whether it may not do more harm than good. Incidentally (or not), most of the excess mortality has occurred in countries implementing lockdown, and following its introduction.
Many people are well aware that “people are dying” (I had seen all of the graphs in your post), but feel that this unprecedented roll-back of basic rights, enhancement of surveillance, loss of employment and looting of the economy by the elites – while we are all shut in at home and unable to protest – is the greater danger.
This crisis is a political issue, and an analysis that ignores the wider context in which it is taking place can only be of limited use. I’m not in the US, but it seems that many people over there are taking what is an objectively extreme position, out of simple knee-jerk opposition to the Bad Orange Man. This clearly is no better than opposing established narratives uncritically.
I very much agree, Ellie. My problem with the post as well, though Denise was certainly thorough in what she chose to cover, but I’m left unsatisfied. Instead of debunking the debunking, how about offer better criticisms of the approved global narrative that’s produced a kind of global lockdown Olympics?
Or, how about question the premise (that this is a big deal). Everyone just assumes the premise is valid in any proportional sense. 300-600K people die of the flu every year. Pneumonia? 2.5 – 4 million. It’s the chief cause of death for children under 5 worldwide. 800,000 children under 5 died in 2017 (latest figures I found in a 5-sec Google). It comes in both viral and bacterial forms and is contagious. How many of you faux righteous virtue signalers wear your Mao Uniform…uh…mask around children under 5? None? Why not?
And the slippery slope fallout from crashing markets–22 million newly jobless in the US alone, millions of businesses trashed globally (many likely never to recover), and hugely complex and fragile supply chains being broken on an hourly basis worldwide–if going to kill an F-ton more people than this bad head cold that can’t even muster a weak flu year worth of mayhem. Expect prices to rise for basic goods substantially. You’ll pay back that stimulus times 100 before it’s done.
Sorry, none of this is even remotely worth saving any of those who died. Moreover, where I’d love to heap sympathy on that as I would flu or pneumonia deaths, I’m resentful and so must honestly say that I don’t give a damn.
Good to see you, Richard! I used to read your blog way back in the Paleo five-finger era.
So, my daughter is a nurse at a hospital in upstate NY, where there is a huge spike in deaths like she hasn’t seen in her 20 years of working there. Most of the serious Covid positive patients are men and heavy drinkers. According to her, they aren’t that fat or old. The ventilators keep people alive longer, but they don’t often make a full recovery afterwards.
If there were no lockdown, this virus would spread more quickly and even more people would fill the hospital. It could weed out the weak alcoholics in the population so we don’t have to deal with them anymore. But you know what? I don’t like that my daughter has to wear a stupid mask for 12 hours, and it puts a rash all over her face, taking care of these guys that might not make it anyway. So I’m with you! Forget the lockdown, if people want to venture out and catch something, they can just stay home and take care of themselves and die at home.
That would be my reply to anyone that doesn’t agree with the lockdown. I’m not saying I agree or not. I don’t know about the economy. But if more people get sick, then triage is absolutely necessary. If you’re over 60, or 50, drink, smoke, and fat don’t bother calling 911. You had life. Let the medical professionals work on people that are more likely to make a full recovery.
Great to hear from you. I don’t get out to other comment sections much, but when I do I hear lots of “used to read your blog,” always makes me feel good and good God, I wouldn’t want anyone to be so die hard that they hang on my words.
So, I actually address some of your points in my counter-post to Denise, here. Specifically, the Mao Uniform … uh … mask, also the cost-benefit in terms of the culling of the old.
Check it out, see if you like:
https://www.freetheanimal.com/2020/04/coronavirus-3-denise-minger-is-thorough-but-misses-the-boats.html
Good stuff.
Hi Ellie,
Thanks for your comments. I don’t disagree. This post was only intended to cover the conspiracy angle (hence “Coronaspiracy edition” in the title), because I think we need to have some sense of what we’re dealing with before we can even begin to assess what types of responses are appropriate. If the whole thing is a hoax, which many have and still do believe, then any reaction is an over-reaction. But it’s not a hoax, even if it’s also not the plague-level crisis some were predicting very early on, which makes the whole thing very complex when it comes to balancing ‘protective’ measures with their unintended consequences. E.g., what would mortality numbers be looking like right now if we hadn’t locked down? At what point do the benefits of slowing down the infection/death rate (such as buying time to figure out how to treat this thing, instead of harming a higher number of people upfront with the wrong treatments) get outweighed by the psychological and economic effects? I don’t know the answers, and to be honest, I don’t even know how this could be parsed. I might write more “editions” related to coronavirus that touch on these topics, but I don’t have confidence in my ability to tackle them.
I do hope the type of questioning promoted in this blog post can (and will) get applied to everything you mentioned.
Anyway, I appreciate your thoughts!
neisy – Your calm, reasonable response is a breath of fresh air compared to the hyperventilating fear-mongering about authoritarian takeover and economic doomsday predictions. I agree with your assessment. It’s not a matter of taking a position but in simply acknowledging how little we know and much misinformation is out there. First, let’s get some clarity and work toward meaningful public debate. Then we can begin to assess what is the most optimal response at this point and going forward.
Another point: yes, it is normal for medical professionals to use reasonable judgement, absent of certainty, to determine cause of death. It is very much more unusual for a specific pathogen to be named in this case.
Any virus is very more likely to be present in the body of a dying person than in the general population.
The countries with the most widespread testing have the lowest lethality rates.
https://swprs.org/a-swiss-doctor-on-covid-19/
Also, on autopsy of old folk who died of a respiratory infection, usually several viral infections are found in biopsy as well as bacterial infections.
I have no problem is the general assumption that in many cases, C19 was the straw that broke the camel’s back. But, that’s the case with a common head cold too, and on a daily basis.
In these instances I’m far more comfortable with saying C19 contributed to death, rather than caused death.
It’s so great that you’re back Denise-we really a breath of fresh air here! Also, I would love it it you would investigate the connection between the virus and ACE-inhibitor blood pressure medications, like lysinopril. People taking these meds are already subject to the exact same symptoms of the virus-dry cough, headache, fever, trouble breathing from swollen airways, with can be fatal unless the drug is stopped. In the last year, 35 million more Americans became eligible for these drugs because they lowered the threshold of high blood pressure. Now, almost half of adult Americans are taking blood pressure meds, and ACE-inhibitors are the front-line meds. Over a month ago, Dr. Fauci noted the connection between ACE-inhibitors and virus deaths, as 75% of those who died in Italy had hypertension, so he was looking into it “very carefully”. African Americans are more prone to the ACE-inhibitor side effects, plus they have more hypertension and are more likely to be taking ACE-inhibitors, as they are the cheapest. Strangely, just as the virus started in a venomous snake before going to the bat (hence the swelling), ACE-inhibitors are also made from snake venom! So, this is a clear path to preventing at least the excess of flu deaths from ACE-inhibitors, because they don’t take them off of this drug when flu patients go to the hospital, but continue to feed the airway swelling! Directly addressing this “elephant in the room” would likely change this from a pandemic to a typical flu, so we need to act ASAP. And, Denise, I think you’re up for the challenge!
https://www.bmj.com/content/345/bmj.e4260
Somehow this came to my inbox although I don’t remember reading your essays previously. Your writing is enjoyable and clearly shows your thought process and advances your thesis. Thanks for sharing. I look forward to reading other items from your archive when I’m off next week (busy at the hospital this week). Thanks!
It’s great to hear from you once again. The timing is perfect for my current discussions and you are the backup needed. Please do write on your crazy past few years and the loss of faith in nutrition as a frontline healing approach.
I was a C-19 sceptic until i caught the damn thing, and three weeks later I am still recovering. I can easily see how more vulnerable people can die either directly or indirectly from this. Yes, we need to be vigilant about how certain government systems could take this C-19 ball and run it into a very weird place, where rights and freedoms are taken away. But for those who don’t believe it at all, I can assure you it’s out there and it’s a nasty piece of RNA.
So sorry to hear, and very glad you’re on the mend! A very healthy young friend of mine caught this as well and has been fighting it for a month.
You lost me. Claim 3, for example, is not at all hard to check and there is nothing to debate. People just need to read the definitions. ROFL They are clearly stating that anyone who dies with a covid19 positive test is included in the death rate. It doesn’t say if they die of covid19. It ways anyone who dies and has tested positive for covid19. They could be in a car accident. I think the problem is that people don’t read. If you pull up the definitions for your state DOH they will tell you very clearly what their stats include, despite whatever the WHO is doing. People just need to look at the little link with asterisk in my state that says for explanation of stats click here. They also define hospitalization numbers for each county as anyone who has been hospitalized, and clearly state they do not know the number of current hospitalizations, only the total number hospitalized so far at any time due to covid19. Florida is doing it this way:https://fdoh.maps.arcgis.com/home/item.html?id=8d0de33f260d444c852a615dc7837c86
Hi Rose,
It may not be hard to check, but few people bother to do so. As for the rest — the murkiness of how COVID-19 might be getting assigned is what makes it important to look at overall mortality, as covered in #4, and which gives a better picture of whether this disease is taking excess lives.
Thank you for the link!
No, wrong again, Denise. Total of excess mortality will get us nowhere because I assure you that at the end of the year total deaths will be down because of the self fulfilling prophecy in play. You literally have billions of people worldwide NOT out exercising freedom, under house arrest, because IT SAVES LIVES!!!
Sure it does. So does locking everyone in a jail cell. Fantastic way to mitigate all sorts of common life risks. Let’s do it, since that seems to be the ONLY standard of value people are taking into account.
Go to the EuroMomo.eu site, look at the charts for 65+ and all ages. How come the spikes in 2016, 18, and 19? Moreover, how come even though the amplitude is similar with 2020, look at how long it lasted compared with the quick way in which this is playing out.
Richard Nikoley – I can’t speak for other places. But in this community, I’ve seen more people outside and exercising than I’ve ever seen in my entire life. The population might temporarily be healthier for all this free time at home, specifically as it is happening with the warm weather of spring. I know I’ve been outside in the sunshine building up my stores of vitamin D.
Also, with so many people at home, more people are probably cooking their own meals than has happened in recent history. Gardening is also experiencing an uptick with gardens selling out of plants as quickly as they come in. At least some of that will be vegetable gardening. The situation has also led local farmers to become more assertive in getting their product to local communities.
On top of that, pollution has gone down. Air pollution does lead to health conditions that are comorbidities of COVID-19. But one study also found that the genetics of SARS-CoV-2 was found on pollution particles, specifically in the Italian cities with high infection and mortality rates. A temporary dip of pollution could do wonders for public health, but of course it will go back to normal quite quickly once industry and driving returns to previous conditions.
There are, as you argue, some people dying who would’ve died anyway. So, mortality rates in the coming years could be lower. Then again, COVID-19 might cause many secondary health problems that could increase mortality for those who otherwise would not have died. It’s hard to know the net result of all this.
Your writing is so brilliant that my head is starting to hurt. This was amazing.
Wow—this is really well done. As a practicing physician you hit one nail right on the head…who do these conspiracy theorists think we supposedly get our marching orders from? If we our part of some vast Left/Right wing conspiracy myself and my partners missed the memo. Filling out Death Certificates has always entailed guess work whether it is presumed heart disease, sepsis, pneumonia, etc. And as you point out, there is more guidance with COVID than other disease state. And I would bet my colleagues—Republican, Democrat, Liberal, Conservative, Pro-Trump, Ant-Trump, etc (they are all the above)—are all kinda doing it the same: to the best of our ability and training with the information available. Anyway, keep up the good work.
You do not have to be an active part of the conspiracy theory you just have to be lower rank obeying orders which by and large doctors do. Take for example the McGovern report and sat fat causes heart disease. We have spent 50 years suffering from this political decision and it is only in the last few years that some doctors are putting their heads above the parapit and citing doubt. Few did this before and still do today because to question the wisdom handed down from above means dismissal or career reprimands. So in conclusion to control an industry like the medical industry you do not need all doctors on board, you just need to control the upper echelons of power
I would love to know what you’ve changed your mind about since you wrote Death by Food Pyramid.
Hi Peter,
I’ll definitely be blogging about this in the near future!
Thank you Denise! You are my favorite researcher/writer, both for the exceptional quality of your work, and for your delightful presentation. I do wonder if you are preaching to the choir – would sloppy thinkers and conspiracists even be attracted to your precision research? I will benefit from your list of self-check questions at the end of the article. Confirmation biases are very hard to see in ourselves, and these questions should help to reduce that hazard. I’ll add my vote to others who would love to read your evolving thoughts on the other “sundry” items you tickled us with at the beginning of this article.
But what if we accept the data?
Overall mortality rates as of the morning of April 17th from worldometers.info for:
World
USA (locked down)
Spain (locked down)
Sweden (not locked down)
I’m using dead/population for death rate. Could also call it probability of dying from covid19.
Pop dead rate (probability of dying from covid19) rate (probability of not dying from covid19)
World 7778393528 148,641 0.0000191095 0.9999808905
Spain 46,754,778 19,315 0.0004131129 0.9995868871
US 331,002,651 34,641 0.0001046548 0.9998953452
Sweden 10,099,265 1400 0.0001386239 0.9998613761
Assuming we are half way through this, I’ll double the numerator for an estimate of the total when it’s over:
Pop deadx2 rate (probability of dying from covid19) rate (probability of not dying from covid19)
World 7778393528 297,282 0.0000382189 0.9999617811
Spain 46,754,778 38,630 0.0008262257 0.9991737743
US 331,002,651 69,282 0.0002093095 0.9997906905
Sweden 10,099,265 2800 0.0002772479 0.9997227521
So what death rate justifies the media/government induced panicked response we are seeing?
And what is the cost in terms of just body count alone? There’s been a huge spike in the number of suicide help center calls. Reported as 800% here: https://fox17.com/news/local/feeling-the-pressures-of-the-pandemic-suicide-hotlines-see-800-percent-spike-in-calls
If there’s a proportional increase in actual suicides, which death toll will be higher? Is our response saving any overall lives?
Yes, people are dying and it’s horrible but during the plague the world’s population decreased my 20%. So far with coved-19 the world’s population has increased more than 10,000,000 in the last two months.
I personally don’t think the means are justifying the end. But maybe I’m just cherry-picking data to because of my lack of critical thinking skills.
Whether the reaction is justified is a separate issue from whether the whole thing is a hoax and the conspiracy theories are valid. The same critical thinking we need to use for “alternative narratives” should be used for all other angles of the situation as well, IMO, including both mainstream and non-mainstream ideas about how to respond. 🙂
That’s quite a qualifying statement you made there.
How are the two unrelated? Under certain circumstances they are completely related. Must I remind you the institution enforcing these draconian edicts and reporting these false numbers are the same? That’s called related.
It’s this total brushing off of possible scenarios which is troubling. I could provide an infinitely long post listing the number of lies and proven collusion brought forth by just the American govt. That would make me a conspiracy theorist though – the single most intellectually lazy term ever invented.
Thanks!
Denise, a very welcome back! Great piece of work, per usual.
That was a nice, detailed analysis. I appreciate your taking the time and effort to write it up. But I wanted to respond to something else that came from the beginning of your piece.
You wrote about your “loss of faith in nutrition as a front-line approach to healing” and then, in the next paragraph, you began with, “But then COVID-19 happened”. I immediately noted the obvious connection.
If anyone doubted the importance of diet to health in the past, this pandemic reaffirms it as a priority. The leading comorbidity is diet-related metabolic syndrome. And so, in multiple ways, this pandemic shows how central is diet to public health.
But what if we accept the data?
Using the CDC/WHO’s data, here’s a comparison of mortality rates as of this morning (April 17th) from worldometers.info for: the World, USA (locked down), Spain (locked down), Sweden (not locked down). I’m using dead/overall population for death rate. Could also call it the probability of catching and dying from covid19.
World
Pop 7778393528
dead 148,641
death rate. 0.0000191095
live rate 0.9999808905
Spain
Pop 46,754,778
dead 19,315
death rate. 0.0004131129
live rate 0.9995868871
US
Pop 331,002,651
dead 34,641
death rate. 0.0001046548
live rate 0.9998953452
Sweden
Pop 10,099,265
dead 1,400
death rate. 0.0001386239
live rate 0.9998613761
Assuming that we are half way through this, I’ll double the numerator to estimate the final rates.
World
Pop 7778393528
dead 297,282
death rate. 0.0000382189
live rate 0.9999617811
Spain
Pop 46,754,778
dead 38,630
death rate. 0.0008262257
live rate 0.9991737743
US
Pop 331,002,651
dead 69,282
death rate. 0.0002093095
live rate 0.9997906905
Sweden
Pop 10,099,265
dead 2,800
death rate. 0.0002772479
live rate 0.9997227521
So what death rate justifies the draconian governmental response we are seeing? Is this style of locking down changing the rates enough to justify the cost? See Sweden’s rates?
And what is the cost in terms of just body count alone. There’s been a huge spike in the number of suicide help center calls. Reported as 800% here: https://fox17.com/news/local/feeling-the-pressures-of-the-pandemic-suicide-hotlines-see-800-percent-spike-in-calls. If there’s a proportional increase in actual suicides, which death toll will be higher? Is this response saving any lives overall? What about the non-fatal mental health fallout from the effects of the unemployment and failed businesses?
Yes, it horrible people are dying but during the plague the world’s population decreased my 20%. So far with coved-19 the world’s population has increased by more than 10,000,000 in the last two months.
I personally don’t think the means are justifying the end. But maybe I’m just cherry-picking data because of my lack of critical thinking skills.
Will you be doing later posts about your “grand explanation”? I am interested in reading about the things you mentioned. (Also, this was a very helpful post for me. Thanks for doing it.)
Hi Marion,
Absolutely! I’m a horribly slow writer, but hope to have something on this up within the next few months. 🙂
I would love to hear your thoughts on normal deaths in nursing homes vrs what we are seeing now. I did a little research and it seems from data I looked at that theCOVID 19 deaths are a fraction of normal deaths, but I may not have had the best data.
Thank you. Great article!
Hi Dan,
This would be really interesting to look into. I know nothing off the top of my head, but if I find any interesting data I’ll let you know. 🙂
While you make a compellingly strong case, Denise, others remind us that correlation doesn’t always mean causation, and that, for example, harm from prolonged ventilator use may be a confounding factor. Moreover– in related news: Many of the Washington elite– even now– are crowded together at the podium in press conferences. I guess “social distancing” is only for the plebian class, huh? “Things that make you go: ‘hmm…’.” #DoubleStandard hello?
Also, prolonged shutting down the economy is very stressful and thus bad for the health.
Indeed, shutting down the economy may kill far more than any virus we see. Just a thought logged in the category of “pros” vs “cons” of our possible over-reaction.
Gordon Wayne Watts in Plant City FLORIDA
Gordon: I agree. The response is far out of proportion to the threat. Very damaging, not only to the economy, and thus everyones livelihood, but social distancing is a terrible seed to plant in everyone’s mind. This won’t end well, given the percentage of our population who have become sheep.
Hi Gordon,
I wouldn’t be surprised if ventilator use ends up contributing to excess mortality, though I have no idea to what degree that would be the case. I think whatever effect is there will be easier to see in hindsight, unfortunately!
Here’s a conundrum: hospital workers will obviously be doing what they can to treat severely ill patients. If the stuff that seemed most logical in the beginning of this whole thing (ventilator use, hydroxychloroquine, etc.) turns out to actually have been harmful, then people who got infected early on were at a much greater disadvantage than anyone who gets infected later. Slowing down the rate of infection (via controversial lockdown measures) theoretically buys us more time to figure out treatments that work instead of shooting in the dark and potentially hurting or killing people in the process. So, there’s an interplay here between the virus and our knowledge of how to treat it that’s time-dependent, and factors in to the whole “what’s the appropriate response?” debate. Lots of moving parts. Thanks for your insights. 🙂
Thx 4 replying, Denise. I recall that I posted 3 comments in total (not counting this one), and you seem to have a lot of responses. I have nothing further to add on this now — except to point out that the sheer number of comments gives me the idea that you may have not seen all of them. It can be tough keeping up with new comments — and hope that you have some “method” in place to make sure that when a new comment appears, you don’t have to look for it as a needle in a haystack — or something like Facebook where you can see which comments were “read.”
My point is that it’s optimal for you (as the author and a well-known personality) to be able to see (and respond to, if you want) all comments — but in a way that makes sure you don’t have to do anything more than look at new comments. Since there is both email notification and the web blog here, itself, those are 2 methods, and maybe software exists to keep track of which comments were read.
Thx for the community discussion. My latest (3rd not counting this one) thought was that this is a real danger but not as bad as some past epidemics. Only my guess, but that’s better than nothing.
Oh, the virus is real for sure. And it’s definitely killing people.
The question is: is it natural or was the precursor made in Fort Detrick then transferred to the Wuhan BSL-4 Lab in China as part of a joint research agreement, from which it escaped? This sort of research would allow China to test a new vaccine to protect against a weaponized coronavirus.
When dealing with viruses, it’s good to learn a bit about bioweapons research. This sort of research, which is common around the world, is itself making a bioweapon; the excuse given is “we need to make the weapon in our labs so that we know how to defend against it.” This isn’t wrong but everyone is using the same excuse, which is why there are 60 BSL-4 labs in existence or being planned, with 13 existing or planned in the US alone. The list below is from a 2013 page by the Federation of American Scientists (https://fas.org/programs/bio/research.html#USBSL4). The CDC operates 2 facilities.
Centers for Disease Control and Prevention
Atlanta, GA
Center for Biodefense and Emerging Infectious Diseases
University of Texas Medical Branch
Galveston, TX
Center for Biotechnology and Drug Design
Georgia State University
Atlanta, GA
Southwest Foundation for Biomedical Research
San Antonio, TX
Rocky Mountain Laboratories Integrated Research Facility
National Institute of Allergy and Infectious Diseases
Hamilton, MT
United States Army Medical Research Institute for Infectious Diseases
Department of Defense
Frederick, MD
Integrated Research Facility
National Institute of Allergy and Infectious Diseases
Ft. Detrick, MD
Galveston National Laboratory
University of Texas Medical Branch
Galveston, TX
National Biodefense Analysis and Countermeasures Center
Department of Homeland Security
Frederick, MD
National Bio- and Agro-Defense Facility (NBAF)
Department of Homeland Security
Manhattan, KS
National Biocontainment Laboratory (NBL)
Boston University
Boston, MA
Virginia Division of Consolidated Laboratory Services
Department of General Services of the Commonwealth of Virginia
Richmond, VA
Tell me again why the US needs this many Biosafety Level 4 labs?
In other words, EVERYONE—including and especially the United States—is breaking the bioweapons treaty by calling it “defense research.” If you don’t get that, you’re missing a major element of the new arms race and why China wanted its own BSL-4 lab, which just happens to be located in Wuhan.
As an aside, an unfortunate side effect of vaccines with these sorts of viruses is pathogenic priming (Fauci and others call it “immunological priming” but it’s the same thing). After the vaccination, subsequent exposure to the wild virus causes more harm than good. Very useful in a bioweapon, by the way, and what you absolutely want to avoid in a vaccine.
For more on pathogenic priming and why no one should wait for a vaccine, see:
“Homology between human and viral proteins is an established factor in viral- or vaccine-induced autoimmunity. Failure of SARS and MERS vaccines in animal trials involved pathogenesis consistent with an immunological priming that could involve autoimmunity in lung tissues due to previous exposure to the SARS and MERS spike protein. Exposure pathogenesis to SARS-CoV-2 in COVID-19 likely will lead to similar outcomes.”
Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7142689/
Ok, back to the source of the virus. Lots of people are looking at the viral sequence and saying, “No way this level of mutation happened in one shot in nature. This is man-made.”
Fox is chasing this down but their angle is “[this wasn’t bioweapons research but] part of China’s attempt to demonstrate that its efforts to identify and combat viruses are equal to or greater than the capabilities of the United States.”
Sources believe coronavirus originated in Wuhan lab as part of China’s efforts to compete with US
https://www.foxnews.com/politics/coronavirus-wuhan-lab-china-compete-us-sources
Whatever you say, country trying to catch up to the US in the bioweapons arms race.
And TWP reported that the safety practices at the Wuhan lab are inadequate:
State Department cables warned of safety issues at Wuhan lab studying bat coronaviruses
https://www.washingtonpost.com/opinions/2020/04/14/state-department-cables-warned-safety-issues-wuhan-lab-studying-bat-coronaviruses
I was so excited to see a new post, and this one didn’t disappoint me. It’s wonderful to have some COVID clarity.
I have a question about those weekly death graphs. Why does the death rate fall during December and peak in January?
Could it be true that people on their death bed want to see one last Christmas and new year, and so use their death defying powers to live on?
Or is December a safest time of the year, and January the most dangerous?
It can’t be that the data crunchers just didn’t get around to entering their data because they were Christmas shopping, and then were overwhelmed with work in January, and made mistakes?
Why?
Really well done. Thanks for putting this together.
Craig
________________________________
Thanks so much and good to hear from you.
If you remove the deaths in nursing homes, this is just a bad flu. They didn’t flatten the curve, they caused a run on the hospitals, and spiked the deaths into a 30 day period. New study:
https://www.medrxiv.org/content/10.1101/2020.04.14.20062463v1?fbclid=IwAR3rBMR1buESozHYuzHvFMzfk8V22MArO8c8nEbAIxE0-uhjyJJB5EOD_88
“These prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50-85-fold more than the number of confirmed cases.”
Hi Robert,
That study has some pretty severe issues that make its findings hard to trust (a good critique is here — https://medium.com/@balajis/peer-review-of-covid-19-antibody-seroprevalence-in-santa-clara-county-california-1f6382258c25). The most glaring problem is that they recruited people via Facebook ads and very likely ended up with a sample skewed towards folks who’d had COVID-19 and wanted to get a free antibody test — much less likely for someone who hadn’t been sick to see the study and go through the effort of volunteering. The accuracy of the findings depend on the sample being representative of the population. Likewise, they used an unapproved antibody test, largely took the manufacturer’s word for its accuracy/sensitivity, and as far as I know there isn’t data on its cross-reactivity with other coronavirus strains.
Seattle is doing antibody testing as well and the results of that will be helpful to compare against, at least for US data.
Great piece, thank you. Now, I am Italian but I live in Spain. As you showed, the excess number of deaths has just dropped to normal boundaries, for pretty much any region. However, we are still having, in Spain, 500+ COVID deaths per day. Would these people have died anyway? My tentative answer is yes. What do you think?
Hi Laurenç,
Thank you! It’s very possible, although data from this most recent week is shaky due to Easter causing a delay in death registrations (this seems to happen around most holidays). If next week doesn’t show elevated mortality compared to this one, I’d say either your speculation is probably right, or we’re seeing the aftermath of people in poor health getting wiped out early in the pandemic, and who are therefore not around to die now (to put it very crudely). Data gets updated on Thursdays so we’ll see what it looks like after the holiday influence is gone!
Thanks for another lucid post, Denise.
I buyed your book read by your Dad (great reader by the way!) and now I click for your clickety splick count. You were Missed Miss!
You wrote in the initial paragraph, “my loss of faith in nutrition as a front-line approach to healing.” Before you write off nutrition for healing, I suggest you have a look at Dr. Rhonda Patrick’s videos on the pervasive low rates of micro-nutrient blood levels in most people and the incredible effect that precise supplementation can have on auto-immune diseases including Alzheimer’s disease. She is an absolutely brilliant researcher working at the Children’s Hospital of Oakland’s research lab until the tutelage of Dr. Bruce Ames. Please give it a shot.
This was exactly what I needed to read today. Wonderful article. Thank you for your research and your truth.
Here’s the newest thing that if true, should be a whopper of a revelation.
https://www.medrxiv.org/content/10.1101/2020.04.14.20062463v1
“These prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50-85-fold more than the number of confirmed cases.
“The population prevalence of SARS-CoV-2 antibodies in Santa Clara County implies that the infection is much more widespread than indicated by the number of confirmed cases. Population prevalence estimates can now be used to calibrate epidemic and mortality projections.”
But, this will likely be completely ignored, just as was the perfectly controlled “experiment,” the Diamond Princess where onLY 20% of the the total on board were infected, and of those, fully 60% never had any detectable symptoms.
Doesn’t fit the oh so cherished panic, hysteria, self-fulfilling prophesy, power grab, politicized, social-media driven REALLY EXCITING STORY!!!
Hi Richard,
See my reply to Robert above, who posted this as well. A good critique here — https://medium.com/@balajis/peer-review-of-covid-19-antibody-seroprevalence-in-santa-clara-county-california-1f6382258c25 — their recruitment methods almost guarantee they got a disproportionately high number of folks who had COVID-19, and the false positive risk is significant, which would destroy any ability to accurately scale the findings to the rest of the population.
Based on how widely this paper is already getting circulated, I’d say it’s the opposite of being ignored. After all, the media’s currency is shock, not necessarily a cohesive narrative, and this provides a nice “OMG plot twist!” to keep people on their toes. 😉
More pedantic nit picking from Denise. Got it.
And good God. The range given is 48-81K. You can’t even prolly grant that that’s enough to wash out selection bias via Facebook ads?
The big point is, no matter how they select test subjects there are always significant numbers with antibodies. I think 15% is the lowest I’ve seen.
And the bigger problem is, nobody in Trumps circle of jesters talk about any of this. The premise narrative is never even questioned. I heard Trump say 3 times the other day that his administration’s actions and those of states have saved 2 million lives.
You’re dealing with fucking liars, and that’s why I had to write this:
https://www.freetheanimal.com/2020/04/coronavirus-3-denise-minger-is-thorough-but-misses-the-boats.html
Basically what I just read is a combination of ad hominem anti-conspiracy language, scarecrow examples and arguments, and appeal to technocratic authority with their data and graphs. If the government is going to shut down society then the onus is on them to prove their case and they simply have not.
We must take a step back and ask just how a “virus” with no cellular structure, no ability to reproduce itself and no ability to survive outside the host can be spread in the ways we are being told. In other words, the entire premise of this post – and of the current narrative in general – is untenable. The proper steps required to id a new condition have absolutely not been taken here.
I am much more curious about your views on nutrition mentioned at the beginning. Unfortunately instead you’ve jumped head first into the mire of a subject which is highly questionable and 100% brought forth by government and media; the one-two punch of prevarication. Seems to me what is needed are more microbiologists and less megalomaniacs such as Bill Gates…but I digress.
“how a “virus” with no cellular structure, no ability to reproduce itself and no ability to survive outside the host can be spread in the ways we are being told.” Where did you come by your “knowledge” of viruses? There is nothing about the structure, reproductive behavior, environmental persistence or transmission routes of SARS-CoV2 that is markedly different from other viruses. Yes, they are basically just bits of genetic material. Viruses do not lack the ability to reproduce – they do it quite efficiently by hijacking the cells of the host organism. Many viruses, including this one, survive quite well outside the host organism for hours to weeks. And many spread in identical ways – from bodily fluids of the host organism. So, whence comes the idea that the nature or behavior of this virus is anything out of the ordinary? And whence comes the idea that microbiologists are not involved in the assessment of the virus? Do you not read the numerous articles being published in any number of scientific journals, mostly as open documents so that researchers can share findings, by microbiologists and related specialists? And what on earth does Gates have to do with it?
Are you a microbiologist? You don’t sound as if you are one. I am personally not either so I generally stick with those who do have experience in this area; off the top of my head Dr. Tom Cowen is one I learned a lot from, but I have read of more who agree. He maintains viruses do not have the ability to reproduce themselves, they must reprogram the dna of a host in order to get that done. Viruses are cell specific, meaning they do not even have the ability to spread to another part of the host’s body much less survive outside the host and stay viable long enough to spread.
He also explains in detail why the current pcr test is totally inappropriate for diagnosing anything, skewing pretty much all current data. Even the creator of the pcr test warned it was not to be used as a diagnostic tool. If the current narrative being put forth was correct, then we should be able to draw blood from CV patient and from that blood harvest coronavirus… hasn’t happened even once. There would also exist no variability of symptoms and treatment and those symptoms would be mutually exclusive of other conditions. There are other protocols involved in identifying a new condition which have been conveniently ignored.
It’s unbelievable I still have to explain Bill Gates’ involvement in all this given his Ted Talk speeches and recent media appearances. He is personally funding the development of a mandatory vaccine which is in store for us all and is friends with that weasel Dr. Fauci. Look up ‘Event 201’ which he was involved in. He was kicked out of India because so many children died or were permanently maimed from vaccines he brought forth. Same with Africa. He has openly supported death panels. How is it people are still ignorant to this?
You can go back to sleep now…night, night.
No, I am not a microbiologist, nor did I imply that I was. I am, however, a retired scientist with an advanced degree and a professional registration that spent a 45-year career in a field at the intersection of the life sciences and the physical sciences. I also have a fair amount of practical experience with coronavirus-caused diseases, albeit in domestic animals, not humans.
As far as your “expert microbiologist”, remember that some scientist proved mathematically that bumblebees are aerodynamically unstable and incapable of flying. The bees, being unable to read the equations, do not recognize the “proof”, and fly despite same. Apparently, viruses treat your expert’s hypotheses with the same contempt.
In other words, you know about as much as I. Your appeal to authority and humorous non sequitur regarding the bees cannot mask that fact. Those scientists you referred to were the same guilded type functionaries who are blowing smoke up our a__es about the cerveza virus today; except our entire way of life has been unalterably worsened as a result of them and the dupes who believe them.
You are certainly entitled to believe whatever you want. It does not affect my life in any way whatsoever. If you wish to believe that viruses cannot affect more than one organ in the human body, that they cannot replicate, that they cannot be transmitted in bodily secretions, have at it. I wish you luck with your belief system.
Even after all that effort of writing this post many even in the comments section here have chosen to not be equally skeptical toward alternative views. In times of fear and anxiety, paranoia and conspiracy theory dominates. Many people don’t simply want fair analysis of the data but are looking for greater meaning beyond what scientific analysis can provide.
https://www.washingtonpost.com/opinions/the-dangerous-conservative-campaign-against-expertise/2020/04/09/604d10e6-7a95-11ea-a130-df573469f094_story.html
“Though we are still relatively early in the pandemic, this much seems clear: The medical experts recommended aggressive social distancing to bend the curve of infections and deaths downward. Americans generally trusted the experts. By all the evidence, aggressive social distancing is bending the curve of infections and deaths downward. And places that were earliest and most aggressive in this approach have seen the best results.
“This outcome doesn’t strike me as murky. It is difficult to see how experts whose advice clearly saved tens of thousands of lives can be called discredited. It is easy, however, to see how making this false claim might undermine public adherence to their advice, which still matters greatly in the crisis.”
Not only do you use an openly compromised media outlet as reference, but from the opinion section no less. You may want to stay in the shallow end a little longer. Wouldn’t want you to drown or anything. The only curve which has flattened is average worldwide iq.
I have my own issues with WaPo and Bezos. But it’s no more compromised than the rest of the mainstream media. Anyway, what the author writes would be just as true if it were published elsewhere. Should I instead listen to Alex Jones?
If it were true, you would be correct the source does not matter; but how often is truth present in an opinion piece?
I agree with you, wapo is just as compromised as the rest of corporate/state run media sources, which means you should be extra skeptical of all and the data brought forth to the point you should assume it is all false.
Read up on the efficacy of utilizing pcr tests for diagnosing this condition, that test is completely unsuitable to this purpose. Rest assured it did not come from Alex Jones (you pulled off a red herring fallacy with the AJ comment by the way). Over 50% false positives diagnosed with the pcr test because of the very nature of this type test.
I am a strong critic of mainstream/corporatist media. But if you sweepingly and mindlessly dismiss everything ever published in mainstream media in knee-jerk fashion, you are unlikely to come to a reasonable, fair, and meaningful conclusion. That is my only point.
I have actually found the opposite to be the case. How many lies will you look past before you actually become a true skeptic? You are certainly not one now regardless of your claims.
You are assuming you know what is true in the middle of limited and conflicting information. I’m not arguing for or against any particular information. I remaining neutral in my skepticism.
Here is the problem. We simply don’t know much at the moment. But if we are wrong, the consequences could be high.
Even if millions of Americans don’t die of COVID-19, if the infection runs rampant without controlling it before we come up with better treatments, millions of Americans could end up with permanent health conditions after surviving infections.
We simply don’t know. Why assume you know what you possibly can’t know at present?
The irony appears to be lost on you that you want us to listen to the prevailing set of experts on the blog of someone (Denise) who has definitively shown (among many, many others now) that the universal expert advice to eat less fat and more carbs is one of the primary causes of a chronically ill population around the world. (With a further irony that this previous advice has made people who followed it more susceptible to COVID-19.)
You appear not to have learned the lesson from the diet debacle: experts are wrong all the time and questioning them should be encouraged.
Regardless of your post (which does have some merit), lots of surveys are coming in now showing COVID-19 death rates below 1%, sometimes as low as 0.1%, about the same as a severe flu season.
See this news article by that hotbed of right-wing conspiracy theory, The Nature Group:
Antibody tests suggest that coronavirus infections vastly exceed official counts
https://www.nature.com/articles/d41586-020-01095-0
If the Stanford study (yet to be peer reviewed) and the others underway provide corroboration, the more widespread nature of the virus leads to the following consequences:
1. The death rate is down around 0.1%—about the same as a severe flu season, which is precisely what Sweden estimated and why they chose not to do a lockdown.
See: Why Lockdowns are the Wrong Policy — Swedish Expert Prof. Johan Giesecke
2. Contact tracing is no longer an option.
“Arnold Monto, a professor of epidemiology at the University of Michigan’s School of Public Health, said “we’re beyond” what contact tracing can offer.
“We have community-level transmission nearly everywhere now. Contact tracing is not going to contribute when you’re seeing mild cases going undiagnosed without the ability to test,” Monto said. “Even in some rural areas, you’re having cases.” ”
That was written three weeks ago on March 26, 2020. See:
It’s Probably Too Late to Use South Korea’s Trick for Tracking Coronavirus
https://www.thedailybeast.com/too-late-to-use-south-koreas-coronavirus-tracking-technique
Contact tracing works only if you start early and you have all the infrastructure in place (sufficient people, sufficient tests, sufficient reagents for the tests). The failure of the US in this regard is almost complete and has stunned the world. The US is now the locus of infections with over 750,000 cases, well ahead of second-place Spain; see https://www.worldometers.info/coronavirus, as of April 19, 2020.
3. Such a low death rate may not warrant the reaction we have taken so far (destroying millions of people’s livelihoods, driving up domestic abuse, driving up suicides, driving up poverty) or the contact tracing or a mandatory vaccine.
“UNITED NATIONS (Reuters) – Hundreds of thousands of children could die this year due to the global economic downturn sparked by the coronavirus pandemic and tens of millions more could fall into extreme poverty as a result of the crisis, the United Nations warned on Thursday.
The world body also said in a risk report that nearly 369 million children across 143 countries who normally rely on school meals for a reliable source of daily nutrition have now been forced to look elsewhere.”
U.N. warns economic downturn could kill hundreds of thousands of children in 2020, April 16, 2020
https://www.reuters.com/article/us-health-coronavirus-children-un/u-n-warns-economic-downturn-could-kill-hundreds-of-thousands-of-children-in-2020-idUSKBN21Y2X7
Once more of the population hears this sub 1% number, the will to support any of these measures will crumble. Protests have already begun in the US and they will continue to spread. People are at home and they are watching this very closely. This sub 1% number will become common knowledge.
“Rallies in Arizona, Colorado, Montana and Washington state were expected on Sunday, following earlier protests in half a dozen states.”
Coronavirus: US faced with protests amid pressure to reopen, April 19, 2020
https://www.bbc.com/news/world-us-canada-52348288
The data are certainly heading in one direction: the curve has been flattened, time to re-open the economy and do our best to protect the old and vulnerable. In my view, we have passed the point when the treatment is worse than the disease.
Unlike some but like Minger, I’m an equal opportunity skeptic. Not everyone appreciates such skepticism, but that’s how I roll.
We simply don’t know a lot now. But the safe bet is to delay the spread of the disease to buy some time until we know more. As Minger has said, it’s best to delay most of the infections to a later time when hospitals won’t be overwhelmed, supplies are stocked up, and better treatments are available. We are in the dark at the moment.
The next phase might be slow to come. A vaccine could take years to develop. Many vaccines take a decade or longer. And with some viruses such as AIDS, no vaccine ever resulted despite massively funded research worldwide. We can’t rely on necessarily getting a vaccine any time soon.
As for herd immunity, that would require 60-80% of the population to become infected and recover. Testing shows some countries at around 10-14% recovery rate so far with it returning in fall. It could take several repeats each season of many years before herd immunity is achieved. But at this point, we aren’t even sure how immunity works with this virus.
“But the safe bet is to delay the spread of the disease to buy some time until we know more.”
This is true only if the further damage from a shutdown is tolerable AND this is as serious a disease as it was once thought. If either were true, neither is true at this point in time.
== If We Continue, We Are Heading into a Depression Worse than The Great Depression ==
Indications are that further damage is not tolerable. In the US we have 20+ million people unemployed drawing down the almost non-existent savings most have. This is already causing more drug abuse, more domestic violence, more suicides. It’s probably already too late to stop the US poverty rate from increasing, possibly dramatically, especially if 47 million eventually lose their jobs over the summer.
““Low-income and poor people face far higher risks from the coronavirus due to chronic neglect and discrimination, and a muddled, corporate-driven, federal response [that] has failed them”, said Philip Alston, the UN Special Rapporteur on extreme poverty and human rights, who made a fact-finding visit to the US in 2017.
He painted a picture of record layoffs, a weak safety net, and a Government “focusing primarily on businesses and the well-off”, saying that significant portions of the country “will soon face destitution unless Congress takes far-reaching action”.
Over a four-week period, more than 22 million people have filed for unemployment and US Federal Reserve economists reportedly project up to 47 million lost jobs through the summer.
Moreover, food bank use is skyrocketing and almost a third of housing tenants in the US reportedly did not pay April’s rent on time.”
US must improve COVID-19 strategy to keep tens of millions from falling into poverty, urges rights expert
https://news.un.org/en/story/2020/04/1061982
And, as usual, these circumstances affect the poor much more than people who have some buffer, such as the middle-class. This will have essentially no material impact on the rich.
What is happening here is that we are getting a delayed signal from our actions. It takes many weeks for a job loss to manifest into, say, homelessness. People are unable to see the train barreling toward us but the train is undoubtedly already rolling and picking up speed.
Covid-19 Could Push Half A Billion People Into Poverty
https://www.statista.com/chart/21382/poverty-levels-due-to-a-coronavirus-recession/
With the current strategy, by the time we stop the lockdown, we will be in a full depression with tens of thousands of bankrupt businesses.
As for the disease severity, I addressed that in my previous comment: all recent indications are that it’s going to come in far lower than the original estimates.
It’s time to change strategies and there is no time to lose.
There are smart ways and not so smart ways to go ahead. It’s not a black and white situation of either close the whole world down or entirely open everything up.
The partial closures, varying by country and state, are simply a temporary measure until we have better info and responses. Taking action based on ignorance and assumption is not wise at this point.
But that doesn’t mean we can’t move forward in certain ways. If we could ensure everyone was wearing masks and practicing social distancing as much as possible, the economy could open up much more quickly, especially if testing improved and became more widespread.
Let’s just be smart about it. That is all that is being suggested by the likes of Minger.
Great to have you back, Minger. Even making such a boring subject as COVID-19 interesting. You rock! Looking forward to more posts, about anything really. 😀
Take care.
/S
Very good read. People are dying. One thing I kept waiting for, serological evidence of the denominator. How many people have been infected (particularly the asymtomatic) and now immune. That’s the problem with novel viral infections. We all get sick at once! The Grim Reaper has a spring clean of weak and infirmed. Time to give up the bat soup !
Thank you Denise, for an article both entertaining and very informative.
Please don’t leave it so long to make another post here, please.
You left out the part about the exponential growth that should have started earlier in December or January in the US when 70 to 80 flights were coming out of China to the US. If it was that serious, then you would seen exponential deaths earlier.
Also Can you ask CDC to update its website? Its not aligned with the msm’s and bill Gates narrative that the only way to cure Covid19 is with a vaccine. Cdc thinks you can recover from it by staying at home for 14 days. Who’s right?
https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/steps-when-sick.html
As far as CDC reporting is concerned (and I am not fully aware of its standards), I think just like any other event, instead of jumping to conclusions as you say, these tail risk events should make us more critical of current standards to better improve future standards.
An example would be to report the Cause of Death under General Classifications and then Subclassifications (Where the subclassification could have more interperative leeway).
So if it were Respiratory related That would the General Classification, and the Sub classification could be COVID 19.
If it were Heart Related, We could have Cardiac Classification and then Covid 19 as the Sub Classification.
In this way we can see if we are experiencing an increase in all classifications that would include COVID 19 as a subclassification, and we can also make a judgement as to how confident we are that the medical community is classifying properly (By analyzing the year over year variances in non Covid Sub classifications).
If that analysis shows there was a large potential error, we change the standards/definitions to minimize the error; and for years past, we simply asterick the data with an explanation of the potential range of that error.
Great share! Keep that wonder mind/body churning the butter from the cream!
Excellent read, thank you.
Excellent as usual, but I have questions on the financial incentives to overreport. In general, you don’t seem to address how medical judgement can be impacted due to what reimbursement might be available. In particular, here is an excerpt from the CARES act: “Section 3710: Medicare Hospital Inpatient Prospective Payment System Add-on Payment for COVID-19 Patients During Emergency
Period
Increases the payment for treating a patient with COVID-19 by 20%. This applies to payments made to hospitals for
Medicare patients, and creates a new COVID-19 Medicare code. This add-on payment would be available through the
duration of the COVID-19 emergency period.
Impact: Increases payment for hospitals treating Medicare patients with COVID-19.
Hi Denise! You had me, you really had me…until you used data in the singular. And from an English major no less! 😉
Just kidding (well not about the improper use of “data”). Great post, and glad to see you back on the interwebs after your long hiatus.
These “advanced” Covid-19 tests can’t distinguish between a common cold coronavirus and a Covid-19 coronavirus! What say you, Denise?
https://www.globalresearch.ca/manufactured-pandemic-testing-people-any-strain-coronavirus-not-specifically-covid-19/5707781
https://www.boston25news.com/news/cdc-reviewing-stunning-universal-testing-results-boston-homeless-shelter/Z253TFBO6RG4HCUAARBO4YWO64/
Yep. Even the inventor of the pcr test warned against using it as a basis for diagnosis.
The current statistics for “Covid-19”, as of today, April 19, are: Cases – 2,277,878, Deaths – 148,013. The world is in a state of panic and in lock-down because of those numbers. If the results were: Cases – 0, Deaths – 0, due to “Covid-19”, for they surely are, would the world be in a state of panic and in lockdown? I suppose if Anthony Fauci had his way, it would be. But who in their right mind would consider it appropriate to destroy the world economy, and “imprison” the world’s population due to the result of a laboratory test, a test whose very creator has stated is INCAPABLE of distinguishing between the many coronaviruses that exist in the world? Have the world’s leaders, and the scientists that advise them, lost their collective minds? Hopefully, Tucker Carlson will publicize this issue on his program Monday evening. All the great accomplishments of man over many centuries, to be waylaid like this, to be blindsided like this, reveal what really drives the species: the raw, unthinking emotions of a primitive brain. Rationality be damned. The world has produced many great minds, many great thinkers. Fauci is not one of them.
Steve: That is a case fatality rate of 0.065, a bit more than half the typical influenza CFR of 0.1. What to make of this is hard to say. The test for an active case is PCR, which is very problematic used as a diagnostic tool, and there is not, as yet, an antibody test for this specific coronavirus, to determine previous infection. Denise is right; we’re going to have to wait a year or two to sort this out, but clearly this is an unusual condition, with people falling ill and dying very rapidly at times. Locking whole countries down is not helping anyone. This should be a wake-up call to take better care of our elderly.
I would have never that that the legal system would have a role in this “pandemic”, but I see that it clearly does now. An expedited, federal lawsuit needs to be brought before the U.S. District Court in Washington, D.C. against the CDC (Center for Disease Control and Prevention) requesting a Cease And Desist Order be issued to stop the labeling of all positive coronavirus testing as being the result of the “Covid-19” virus. The urgency of the matter being due to a senseless global panic! Though the world may be experiencing an unusual uptick in deaths, above and beyond the norm as Denise has shown, I would submit that the extraordinary panic that has ensued since this issue came to light is the guilty party. Can panic kill? You bet it can!
I love the idea. But when the judicial branch resides under the same umbrella as the executive branch, it becomes improbable, nay impossible to expect justice as a result.
I think you will appreciate this link, too, Denise. And what’s up with “my loss of faith in nutrition as a front-line approach to healing”? We’re all on the edge of our seats wondering what happened with Denise. She’s gone over to the dark side! https://ttfuture.org/blog/michael/why-coronavirus-will-soon-vanish-overnight
Very interesting report from Bali:
View at Medium.com
Further thoughts:
We know the numerator (number of deaths, and possibly number of “bad” or “got real sick” infections, tho the latter may be conflated with other infections if an EXACT dna-sequencing test for the COVID-19 strain isn’t done– another limitation). But the denominator (total number of infactions– e.g., including the asymptomatic victims– those without symptoms) isn’t known. So, while an unexplained spike in actual deaths (body count can’t be faked) imply that Conservatives aren’t totally right — something’s going on in a bad way, nonetheless, Liberals are exaggerating this: This isn’t as bad as the one that wiped out like 1/3rd the earth’s population!! Remember, a LOT of people are NOW known to have had it AND LIVED!! VERY WELL, I might add– Forest Gump actor Tom Hanks and his wife, both 63 year-old, kinda fat, and definitely out of shape. They’re getting on quite well.
Indeed, both Sweden and California are using the herd immunity method (California on accident, Sweden by design — and on purpose), and Wu Han, China is open for “Business as usual,” including their WET MARKETS!?.. And yet ALL 3 are getting on just fine.
So, in conclusion, this strain is indeed not good for your health (especially, apparently, elderly obese people with a drinking problem who live in unsanitary conditions and aren’t Type-O or Rh-negative in blood type), but we should avoid being paranoid and instead practice Social Distancing, hand washing, Face Masks, and good health measures (eating well, quality sleep, exercise with moderation, fresh air, sunlight, and stress management).
Denise is Back!!!
Denise!
Good to run into you online.
Thanks for sharing your perspective and the work you did.
There’s a lot to argue about if you are up for it. Let’s stand together and hope the UW is right, and we will be ok soon.
How great to see the talented, funny workhorse Denise back at it again, but what a waste of Minger brain power.
Because is not the issue at hand that we should know if the critics were right all along? People such as John Ioannidis https://www.youtube.com/watch?v=d6MZy-2fcBw , Knut Wittkowski https://www.youtube.com/watch?v=lGC5sGdz4kg or approaches such as in Sweden?
Yes there is excess mortality, but would this not have happened anyway within let’s say a year?
We have wiped out the economy with China style surveillance around the corner and vaccines that may not be all too healthy, ready to take the place of herd immunity. In what way would this be in balance with what we have gained?
Would be great to see Denise unleashed on the basis of these questions and while she’s at it regain some trust in nutrition researching the claims coming from China and New York regarding high dose vitamin C. Because not only the approach of the virus may be wrong, also the handling of the disease has received a lot of interesting criticism. From for instance critical care doctor Cameron Kyle-Sidell.
Good luck Denise! We need people like you!
The longest and most detailed post I’ve written at FreeTheAnimal in years.
Ten years ago, Denise Minger came to me with awesomeness, an unlikely takedown of The China Study from the original data set, not the contrived book by T. Colin Campbell.
Instant fame, once I enlisted the help of many others. Speaking gigs, a book deal, etc.
But now, she weighs n on C19 and I think it’s pedantic. Mostly, I think she wants a post that lasts, but this is an immediate emergency (not because of the wimpy virus) whereas, her past excellent work isn’t time critical.
Accordingly, I both praise and criticize.
https://www.freetheanimal.com/2020/04/coronavirus-3-denise-minger-is-thorough-but-misses-the-boats.html
This response post by Richard Nikoley is the height of narcissism and adds no substance to this conversation. It is effectively a hysterical rant outlining his vacation to Asia without any analysis of relevant data, and it ultimately concludes by saying he doesn’t give a shit about anyone else anyway (which is certainly his prerogative but does not inspire confidence that his chosen pandemic strategy would be in the best interest of other people). A bizarre bonus is his book-licking cheerleading for Trump because he is “fucking” us over. Lol, okay boomer.
Having a rational, data-driven discussion about the economic and political ramifications of shutting down entire countries is missing in our current discourse. But, Denise’s original post is clearly not intended for that purpose, and the reality is that there is no way to know how this shakes out. Every single claim made about the virus (whether politically motivated or not) needs to be picked apart and analyzed with the same objectivity that Denise applies in this post. Tackling each hypothesis about the nature of this virus is not missing the forest for the trees, it is about being thorough and minimizing the disinformation that is spread by both sides of the political aisle.
Given that it is now Spring in the Northern Hemisphere I would expect that it is the tail end of your influenza season with the peak having occurred in December-January. Therefore I assume that the influenza has already culled a high proportion of the old and infirm in Europe and North America, the very people who are vulnerable to CV-19. So if anything I’d say that the fatality rate of CV-19 is understated because many of the most susceptible have already been removed from the population. That’s particularly concerning for those of us in the Southern Hemisphere who are only just going into winter and with the flu season yet to come.
A vaccine is going to take 12-18 months (if ever) to develop. We can’t shut the economy down for that long. But before we can open it up again we need to have sufficient PPE equipment to protect hospital patients and staff, ditto for care homes, and aon accurate test that can identify carriers. And for those of us in the SH widespread flu vaccination. At that point we can let the young and healthy resume work while having tight isolation for the most vulnerable people. However from what I read most countries are not in that position, particularly the UK and USA. Read Malcolm Kendrick’s latest post on the situation in the UK. The situation at the moment is bad enough, removing the lockdown at this point would be catastrophic.
Stuart: If you’re considering getting the flu shot, please read this:
https://childrenshealthdefense.org/news/flu-misinformation-and-coronavirus-fears-my-letter-to-dr-sanjay-gupta/
I think this is very timely of Denise. We need to not be sheeple and dig into the details a bit. Some may not like the results of such digging, but it is necessary. Messy, maybe, but necessary. So glad that she has taken the time to do what most are not going to do. Too many thing that don’t add up in the reporting of this pandemic, if it actually really is one. Keep up the good work.
Glad to see that Denise, ‘Death by food pyramid’, Minger is back in the saddle. Here she has done what most are not going to take the time to do, look for some facts. Once we look at teh facts we can see that regular math does not apply, things just don’t add up. Please do not let it be soo long between posts. We need a hit of reality occasionally. keep it up!
Data from around the world show that the IFR is likely to land between 0.1% and 0.36%, according to the Center for Evidence Based Medicine, Oxford University:
“Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR somewhere between 0.1% and 0.36%.*”
https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates
As more data come in, it’s becoming clear that the initial models have grossly inflated the lethality of this disease, according to Prof. John Ioannidis (Update: 4.17.20).
“It’s time to reopen the economy.”
Watch the video to learn the ins and outs of why he says that.
Welcome back! 🤗 This recent blog post may give you pause for thought. https://ggenereux.blog/2020/04/04/covid-19-vulnerability/ Have you heard about Dr. Garrett Smith’s Vitamin A protocol? Would love to know what you make of it! With kind regards, Andrew.
Virus-free. http://www.avg.com
Hello Mrs. Minger! So great to see you posting again! And up to true form – the world really needs it and I was waiting for it. Thank you so much! Christina
Part of the problem is that there are potentially powerful monied interests promoting conspiracy theories, distrust, and divisiveness. This muddies the water. Here is an example of something strange going on with protests in Canada. It makes one wonder who is really behind it and what they are trying to accomplish.
https://pressprogress.ca/meet-the-strange-and-mysterious-group-organizing-anti-lockdown-protests-across-canada/
Define conspiracy theory. It seems the context you are using it (the same context as Ms. Minger is using it) is as an ad hominem. It’s unfortunate how this benign term has been transformed into a weapon of illogic.
I’m not using conspiracy theory in a single way. There are real conspiracies in the world. For example, that article seems to point to some interest conspiring to manipulate people into protests. But there are all kinds of conspiracies out there.
As for conspiracy theories, it’s a mixed bag. My point, though, is that in a reactionary society such as ours conspiratorial thinking becomes yet another tool of manipulation by the very powerful forces conspiring against us.
There is an interesting study related to this. Those who most strongly suspect Machiavellianism in others admit to being more likely to act Machiavellian toward others. To be pulled into that worldview can warp the mind.
Manipulating people to protest is not a criminal act, therefore not conspiratorial. This is where the illogic of it comes in. Regardless of how many ways you use the term, there is only one correct definition; A is A.
When gaps exist between words and their definitions, constructive conversation becomes impossible.
That is a strange comment. Where did you get the idea that all conspiracies are illegal and that if something is legal it can’t be a conspiracy? What does “A is A”, a reference to Ayn Rand’s Objectivism, have to do with the legality of conspiracies? We are definitely dealing with some gaps here.
Most conspiracies are not considered criminal acts. All that a conspiracy means is a group planning something in secret. A surprise birthday party is a conspiracy. Other conspiracies are more nefarious and immoral, but even then not necessarily against the law.
Consider the legalized bribery of the pay-to-play Clinton Foundation or the legalized bribery of giving lucrative lobbyist jobs to retired politicians who served corporate interests. Or look to regulatory capture where private interests manipulate government to their own ends.
As for a darker example, check out how the Lewis Powell memo has been implemented as a covert power grab. Another one is the vast web of influences funded by the dark money of the Koch brothers and Mercer family, such as shown in the investigative journalism of Buzzfeed.
None of those have been prosecuted by the law, as no law was broken. Yet are they examples of corruption of wealth and power in conspiring against the public? Yes. If further evidence came out on some of them, then they might legally cross the line. But as is, they are well within the law.
More mundane examples are Exxon hiding their own research that proved anthropogenic global warming and pharmaceutical companies hiding the data on the side effects of statins, antidepressants, etc. Both are conspiracy theories. Are they illegal? As far as I know, that has yet to be determined by the US court system.
For some reason, many people have odd ideas about conspiracies. It’s rather simple. It just means to conspire. Going by the dictionary definition, it is a joint scheme that is some combination of secretive, illegal, or harmful — that is to say it doesn’t have to include all three possible factors. Secretive plotting, even if entirely legal, whether or not harmless, is still a conspiracy.
I got the idea conspiracies involve illegal acts from the definition of the word conspiracy. You cannot just pick and choose which part of a definition to include. The origin of A is A was Aristotle, not Ayn Rand and the fact you cannot see the connection to my point exposes you. A conspiracy is what it is regardless of what you call it. Atlas Shrugged is playing out before our eyes though. De-civilization resulting from ignorant worshippers of the state.
I didn’t pick and choose which part of a definition. Across numerous dictionaries, a conspiracy is defined as a group planning/scheming that may or may not be illegal. That is the strict definition. If you don’t agree with the definition given by most dictionaries, then we probably don’t have much basis for meaningful discussion.
By the way, I’m certainly not a worshipper of the state. If anything, I’m probably more of an anarchist than you. But not all criticisms of the state are equally valid in terms of being informed, accurate and useful.
I am referring to the common law definition of the word. Your unicorn sandbox definition appears as the forth or fifth option in the regular dictionaries; does not even show up in the legal definition which absolutely requires an illegal act or tort.
I am certainly no anarchist, it simply does not take into enough consideration the low iq masses. AnCap theory provides the best solutions while still avoiding the coercive state. I would imagine your brand is simply psuedo Marxist which is contrary to the stateless ideals of anarchy. My guess is you have a utopian/unicorn definition of that word as well. More contradictory id.
So, you don’t use words as they are defined in most dictionaries and as they are used by most people. Well, that’s a conversation stopper.
No, I am not swayed by the ignorant masses and their media/pr generated definitions. Modern wiki dictionaries are hardly an appropriate source of vocabulary or nomenclature and even in those the unicorn definition is scarce. One must go several options deep to get the watered down version you robotically spew. The rest include the tort element. Common law only has one option which is the one I use. Your appeal to the herd fallacy is comical…and tragic.
Thank you for the data. However, it is beside the point.
The real point is:
Everyone must be free to make their own choices.
Those who are afraid of catching it/vulnerable – choose to stay home and hide.
Those who are not afraid/do not care if they die – feel free to go outside.
I myself do not care if I live one more day, one more year, or 30 more years.
I accept death is a part of life, even my own.
I want to be free, as is my birthright. Your fear of dying does not entitle you to MY freedom.
YOU stay inside and hide. I will live freely. No one is sovereign over me, except myself and God.
P.S. No, I don’t go to doctors and hospitals. They don’t help people, and they don’t have a treatment for COVID-19 anyway. I would never go to them for “assistance” with anything. Look how “helpful” and “successful” they are at treating the other diseases in the US!
I agree 100%. This article has not aged well given the admittedly inflated numbers from the beginning and the inappropriateness of the pcr test as a diagnostic tool and the fact that Koch’s Postulates have not even been used to isolate the “virus” (which is a scientific fiction; look up exosomes for a more accurate description of what is happening).
All this is actually irrelevant given that even if this virus nonsense was accurate it still does not give governments the right to place their boots on the necks of their citizens as has been done.
Of course according to Ms. Minger and her fanboys these facts are considered ‘conspiracy theory’ so not worthy of consideration.
This was written too early on to see what was happened with covid….
I used to go to Mark Handley’s UCL worldwide tracking, but he stopped updating on May 1. I still go to NYT’s 7 day moving average on new cases for trends. But the biggest and best source of information is CDC’s weekly ILI reports.
https://www.cdc.gov/flu/weekly/index.htm
Two things are particularly interesting. The first is % doctor’s office visits for ILI, which includes flu and mild to moderate covid cases. There was a sharp spike around week 12 (about the magnitude of normal flus), but since then the bottom has fallen out. The graphs say it better, but here’s CDC’s text:
“Nationwide during week 21, 1.0% of patient visits reported through the U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet) were due to influenza-like illness (ILI). This percentage is below the national baseline of 2.4%. All regions remain below region specific baseline levels.”
In other words, flu/covid season is over, and has been for five weeks now. The % doctor’s office visits are down to what is expected in mid July. NO ONE IS GOING TO THE DOCTOR FOR THIS VIRUS ANYMORE. It may flare up again next fall, but we know how to deal with it now.
The second interesting thing is pneumonia deaths, which CDC connects directly to covid.These peaked at 15.9% of all deaths in Week 15, versus a normal 7%. covid has definitely taken its toll, and it is as bad as the worst flus. It lagged the spike in doctor’s office visits by 3 weeks, giving us an indication how long it take for it to kill. But since week 15, pneumonia cases have dropped like a rock, and are now at the expected level for week 21.
Many bad things were done which allowed covid to spread in the US the same way it did everywhere else. But I am grateful for the lockdown. In particular, for the cancelling of all the arena sports playoffs in March, when covid was spreading rapidly. Without that, we could very well be at a million deaths.
Now it’s time to go out in the sun and make some Vitamin D.
@ Free Person – “I want to be free, as is my birthright. Your fear of dying does not entitle you to MY freedom.” What about other people’s freedom? Why do you have a right of taking away their freedom in infecting them and threatening their lives? How is it horrible oppression for you to be kind, considerate, and compassionate in simply wearing a mask?
@ Wandering Scholar – “All this is actually irrelevant given that even if this virus nonsense was accurate it still does not give governments the right to place their boots on the necks of their citizens as has been done.” Boots?That seems bizarre. The much more oppressive destruction of rights during the war on terror never elicited this claim of libertarianism from most of the political right.
@ Thomas Quick – “This was written too early on to see what was happened with covid…. […] In other words, flu/covid season is over, and has been for five weeks now.” Yet infection numbers keep rising in many states. Some states have now reached full capacity in their hospitals, the very thing that we were trying to prevent by shutdown. And we are still only in the first wave. People forget that the 1918 flu didn’t kill millions until the second wave later that year.
I’m not one to fear-monger. Nor am I fan of big gov. But much of the criticism and complaints ring false, superficial, misguided, or premature to me. A precautionary principle of reasonable risk reduction doesn’t seem like authoritarianism overreach. Simply wear a mask or face shield and maintain some basic level of social distancing when possible. We don’t need to go from one extreme to the other, from lockdown to a free-for-all. Let’s calm down and take simple steps, until we see how the situation develops.
Dude, if you are afraid of getting sick, then you are free to stay home. Living in fear must be exhausting for you. What you should be fearing is your lack of o2 intake and excess co2/germ intake as a result of that mask wearing.
And just yesterday a Florida restaurant was raided and shut down by armed, jack booted thugs as a result of these mask edicts (they are not laws). Families dining and all. My metaphor may seem exaggerated to matrix dwelling epsilon types, but not to anybody free of the half dozen or so corporations who are responsible for most if not all of your beliefs.
I’m surprised the science on mask-wearing is still so little understood. The evidence shows that fabric masks protect others more than they protect the individual wearing the mask.
That is why you wear a mask in public places in consideration of others with compromised immune systems. As for having a compromised immune system, that is why one would hope others will be considerate enough to value the life of those around them as much as they value their own life.
That is part of a culture of trust that is admittedly lacking in the United States. Many Americans, unfortunately, don’t believe that they should sacrifice anything for other people, not even the most minor discomfort of wearing a mask for a few minutes while in a store. That relates to so much of the dysfunction and divisiveness in American society.
These Americans proclaim freedom, but refuse to respect the freedom of others. This isn’t freedom. It’s selfishness and callousness. We are only free to the degree everyone is free and everyone’s freedom is respected. That means considering not only how others effect you about how you effect others.
So, wear a mask not because a medical expert, government official, or officer of the law tells you to. Instead, wear a mask because you want to be a kind, considerate, and compassionate person. Do so because you are a good person and want to be part of a good society. Do so because you want to support and promote a culture of trust where you can trust others and others can trust you.
At present in the United States, there is no enforceable law to make you wear a mask against your will. You can refuse to wear a mask. But why would you want to intentionally risk the lives of those around you with compromised immune systems? Why wouldn’t you want to take a small and simple action in reducing the risk to help protect the lives of others? The mask is not a symbol of authoritarian power but a symbol of human kindness.
I’m not afraid of getting sick. I’ve always had a strong immune system. But I wear a mask to be considerate of others or what in common parlance is called not being an a**hole. It’sbasic human decency, not to mention compassion toward those less fortunate with a strong immune system. Just because some people in government are a**holes it doesn’t justify you being an a**hole to your fellow citizens in response. We all should be kinder and more considerate. It’s that simple.
I meant to say, “compassion toward those less fortunate without a strong immune system.”
Well Denise is always very readable. But this is just more noise about noise. 1. There are 2 natural substances which render the Covid 19 virus harmless. 2, Both can be used as prophylactics to prevent infection in the first place or keep the infection very mild. 3. Both can be used in megadoses in acute infection to prevent pneumonia or to reverse it. 4. The Chinese know about this and are using intravenous megadoses of one of these substances in acute cases. 5. The Chinese posted up their protocol using this megadose in December 2019. 6. The Chinese have the pandemic under control because of this. 7. The rest of the world ignores this because we get our orders from the American Medical Association/WHO. “Thou shalt not use any natural substance under any circumstance in medicine”. 8. The Chinese didn’t get the memo. They are laughing at us. 9. The Chinese economy is powering ahead while the rest of the world is headed for a greater depression than the 1930. The Chinese are laughing at us.
These are the facts. It’s unbelievable the amount of noise which has been generated around the Coronavirus to obfuscate these facts. See my video “Covid 19 vaccines suppressed” https://youtu.be/PfICxfYM3NU. As per usual Denise will delete my post..
My dear Denise, I´m thrilled looking into the future and see what you are gonna write, when your right brain hemisphere is fully waking up and you will shine the whole of your true-self-potential into this world. This will be true music-magic. Best wishes from my small Azorian Island. I keep watching what happens. Yes. In the end it might be all about psychology. The mind. The matter/story/topic is completely exchangeable. Let´s look over our own over-our-shoulder-looking selfs. Warmly, Dorothee
Denise, the problem is we can’t find out the truth because one side is squashing all debate. Many Youtube and Twitter accounts are being banned for being varying degrees of skepticism about COVID. Now whether or not their arguments are valid in your eyes or the governments eyes I think you would agree this is very dangerous and often counterproductive. Because as soon as something is censored that itself gives it legitimacy because hey if its so obviously untrue why can’t they just argue against it (like you did) instead of using the time old authoritarian tactic of censorship?
There’s also more subtle tactics of censorship. For example if this post was you arguing that COVID deaths were exaggerated and it got traction on social media then you would be pegged as “COVID denier Denise Minger” the media would attack you saying you were a evil racist rightwing white woman who worked as a shill for the meat industry and you also kick puppies to boot. I’m sure a number of your friends would disavow you, your books would be taken off the shelves of bookstores and you wouldn’t be invited to nutrition seminars (assuming this was before your hiatus). There’s been a lot of stuff written about this type of public online shaming or cancel culture. It works great for the government/powers-that-be because its just as effective as threatening to throw people in prison without the backlash/optics.
My point is there’s a enormous amount of direct and indirect pressure to not post anything heterodox about COVID and also a bunch of other topics like gender differences, climate change, safety of vaccines, black lives matter/police shooting statistics, etc. So while I have a lot of trust in your judgement I don’t think you would be able to post something super controversial that you believed to be true here.